










Dissection Type C – Case 2
Clinical Presentation
- 82-year-old female who presented with chest pain (CCS Class III). Referred for staged PCI of LAD/D1 bifurcation.
Past Medical History
- HTN, HLD, CAD s/p PCI, Hypothyroidism
- LVEF 60%
Clinical Variables
- Prior Cardiac Catheterization: Proximal LAD 30-40% stenosis, mid LAD 80-90%, D1 70-80% stenosis with severe calcification of the LAD.
Medications
- Home Medications: Aspirin, Clopidogrel, Rosuvastatin, Metoprolol Succinate, Amlodipine, Enalapril, Levothyroxine
- Adjunct Pharmacotherapy: Clopidogrel, Bivalirudin
Pre-procedure EKG

Angiograms
1 of 15
Right coronary artery (RCA) angiography 50-60% proximal RCA lesion.
2 of 15
Left coronary artery angiography 30-40% proximal and 90% mid…
3 of 15
Rotational atherectomy of the LAD using a 1.5 mm…
4 of 15
Angiography of the LAD after rotational atherectomy showing slow…
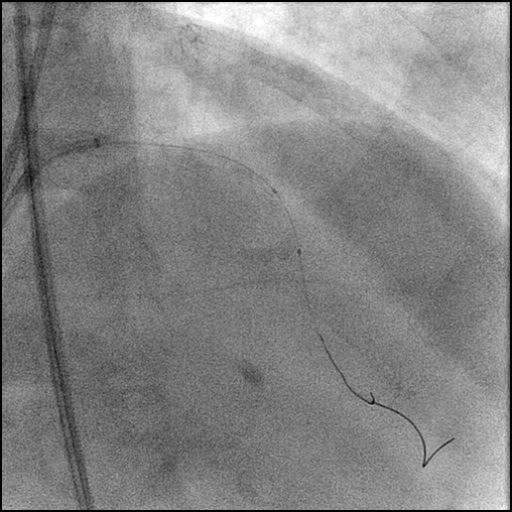
5 of 15
Pre-dilatation of mid LAD lesion with a Trek 2.5/15…
6 of 15
Positioning of a Trek 2.5/15 mm balloon in the…
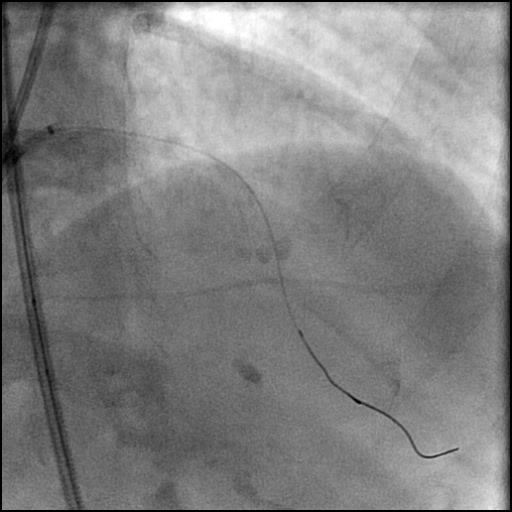
7 of 15
Angiography of the LAD after lesion pre-dilatation showing a…
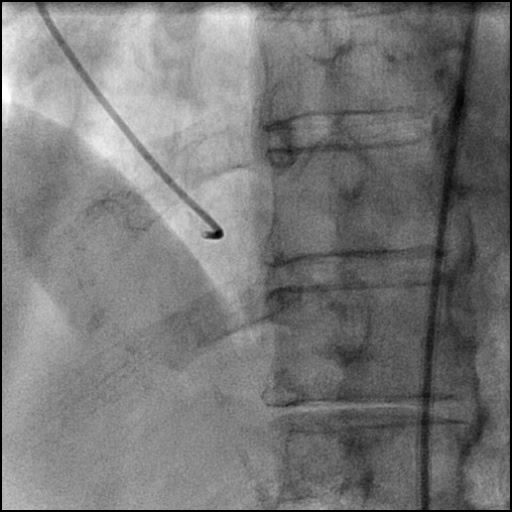
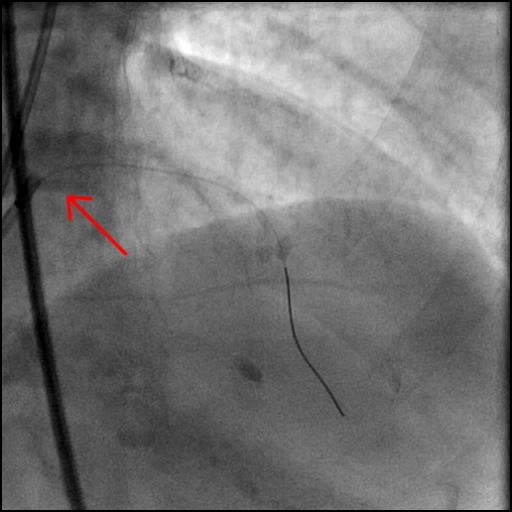
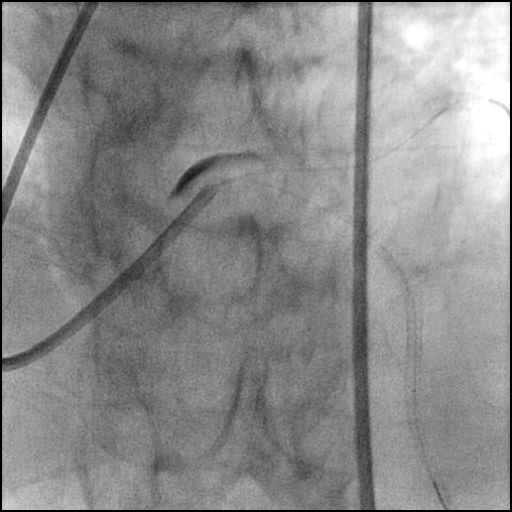
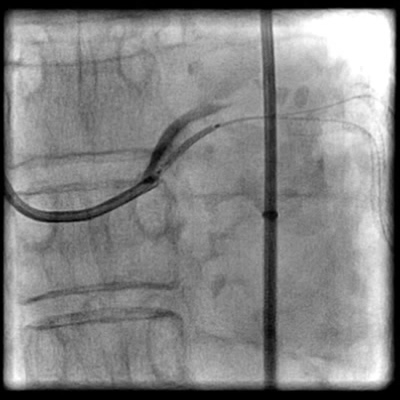
8 of 15
Guidezilla support catheter induced, non-flow limiting Type C dissection…
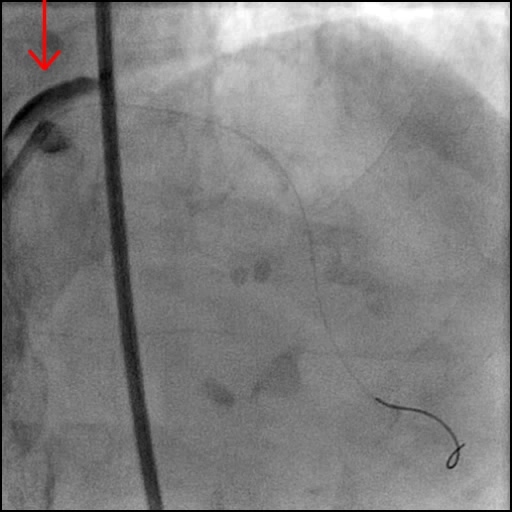
9 of 15
Angiography of LAD after Xience Alpine 2.5/33 mm stent…
10 of 15
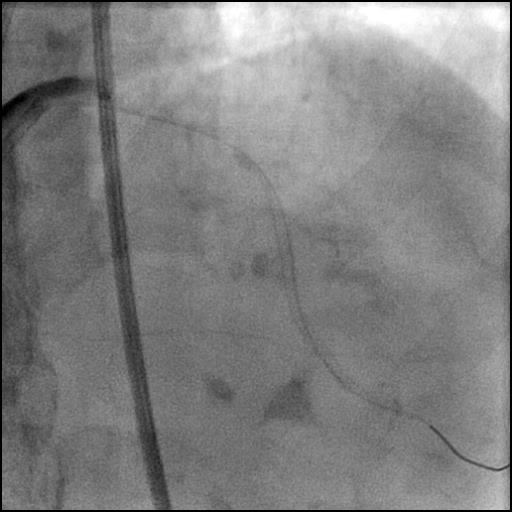
Deployment of a Xience Alpine 3.0/33 mm stent in…
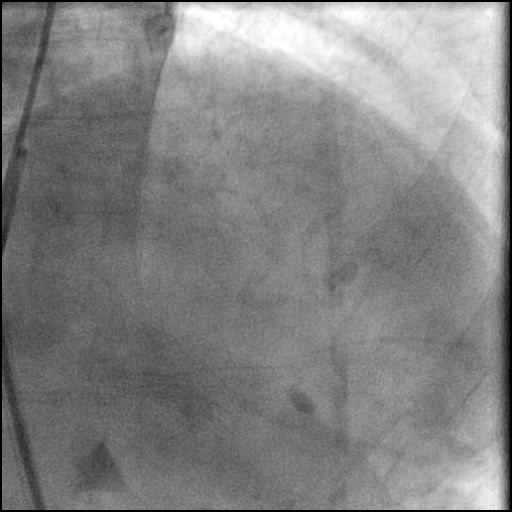
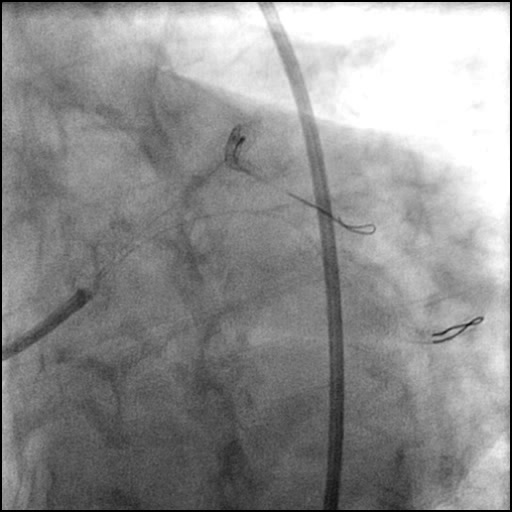
11 of 15
Angiography of the LAD after stent placement.
12 of 15
Wiring of the side branch (LCx).
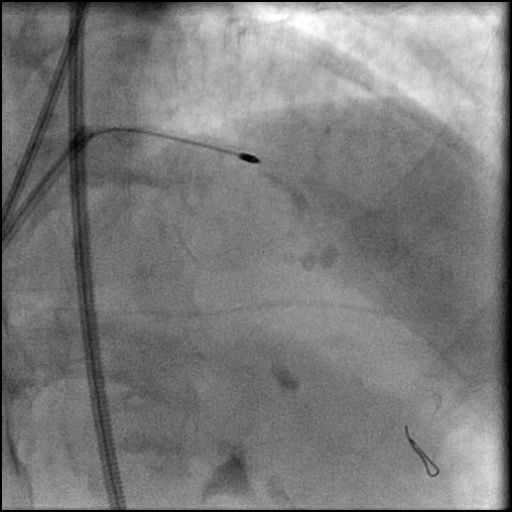
13 of 15
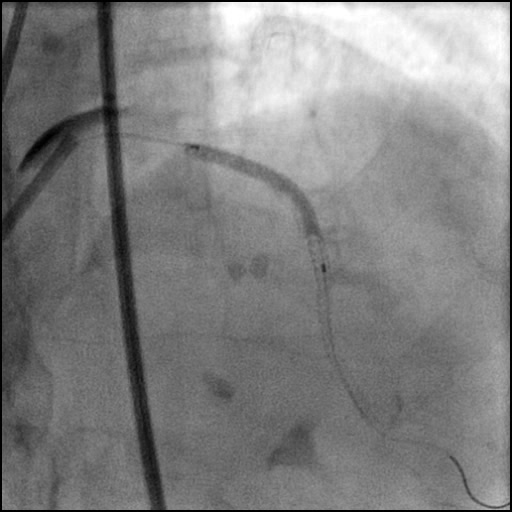
Positioning of a Resolute Onyx 5.0/12 mm stent in…
14 of 15
Angiography of the LM after stent placement.
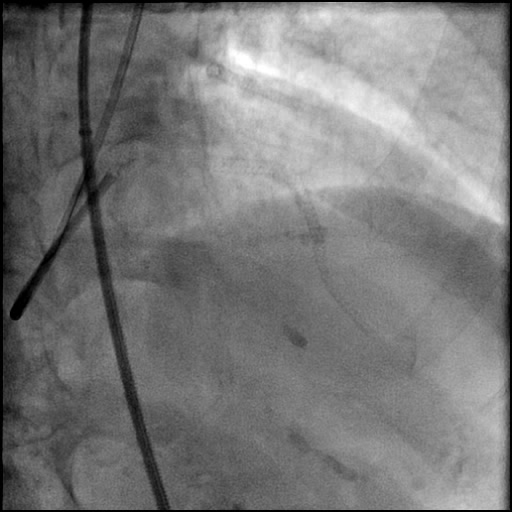
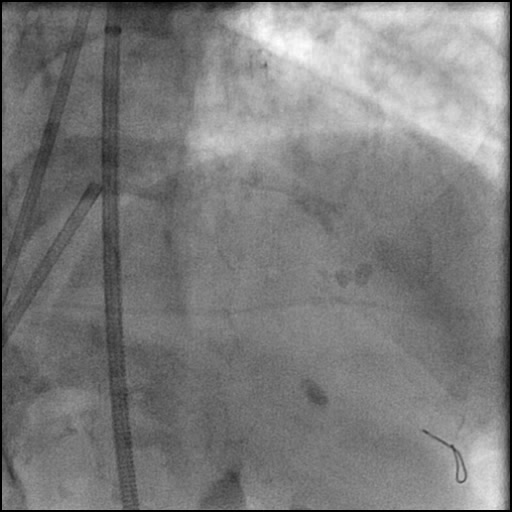
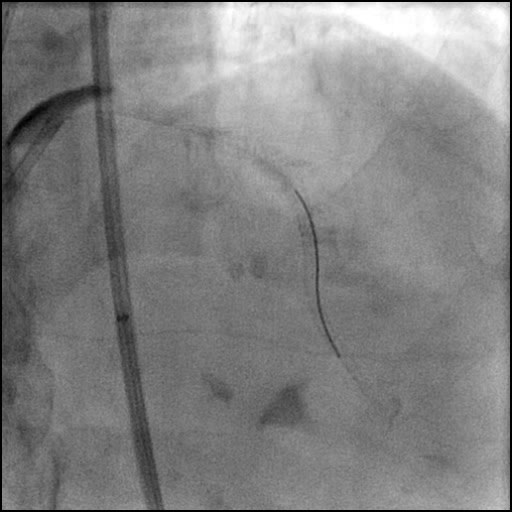
15 of 15
Final angiography showing successful treatment of the LM dissection…
Post-procedure EKG

Case Overview
- Underwent staged intervention of the LAD.
- Procedure complicated by slow flow following rotational atherectomy due to micro-particulate distal embolization.
- This was followed by a Guidezilla support catheter induced, non-flow limiting Type C dissection of the LM.
- In addition, there was significant residual contrast staining with mild retrograde extension of the dissection into the left coronary sinus/aortic wall.
- Procedure was continued and a two stent were placed in the mid to distal LAD.
- Subsequently, side branch (LCx) was wired and direct stenting of the LM dissection was performed with direct placement of a stent, effectively treating the dissection.
- Post procedure, minor EKG changes were noted. However, patient remained hemodynamically stable and without chest pain. Taking this into account along with retrograde extension of the dissection into the left coronary sinus/aortic wall, administration of adjunct pharmacotherapy (Gp2B/3A inhibitor, Cangrelor, etc.) and/or placement of an IABP was deferred.
- Troponin-I peaked at 4.25 ng/mL and CK-MB peaked at 21.0 ng/mL.
- Patient was discharged home two days later without any sequelae.
Learning Objectives
- What is the likely explanation or reason why the complication occurred?
- Type C dissection of an angiographically normal LM due to Guidezilla support catheter injury.
- As contrast was injected through the Guidezilla support catheter, it lunged forward with excessive force injuring the LM and caused a dissection.
- Slow flow due to distal micro-particle embolization during rotational atherectomy.
- How could the complication have been prevented?
- When the Guidezilla support catheter is placed within the coronary it is best to minimize contrast use and administer IC agents with a lower pressure. The outlining of the Guidezilla catheter is coated and more lubricious compared with outer extension guide catheters, therefore making the Guidezilla catheter more susceptible to movement during a procedure.
- What are the important learning points?
- This is a Type C dissection because of the persistence of extraluminal contrast seen well after contrast injection.
- When injecting IC agents/contrast through a support catheter, remember to inject slowly with low pressure. This helps reduce catheter movement which can result in vessel trauma, and if a dissection is present, further propagation of the dissection.
- Dissection of the LM and RCA can propagate both antegrade or retrograde. In this case the dissection extended in both directions. Fortunately, the retrograde extension of the dissection was only minimal involving the left coronary sinus alone. In majority of cases, stenting of the ostium of the vessel involved typically treats the dissection flap preventing further progression.
- If a dissection extends into the coronary sinus/aorta follow up imaging with TEE and/or Cardiac CTA should be performed on a case by case basis. In this case, Cardiac CTA was deferred because of minimal retrograde extension with only the coronary sinus being involved.
- This case was performed during the CCC Live Case Symposium and can be viewed in full with case discussion by clicking on the following link: https://ccclivecases.org/new/complex-coronary/september-2017-ccc-live-case.