










Dissection Type D – Case 2
Clinical Presentation
- 76-year-old male who presented with chest pain (CCS Class III), referred for staged PCI of LAD CTO.
Past Medical History
- HTN, HLD, DM, CAD s/p PCI, ESRD on Dialysis, BPH, Multiple Myeloma s/p Chemotherapy
- LVEF 62%
Clinical Variables
- Stress MPI: Abnormal ischemia involving the anterior, septal, and inferior segments with reversibility and viability; apex is hypokinetic with infarction.
- Prior Cardiac Catheterization: Mid LAD CTO, successful PCI of RCA.
Medications
- Home Medications: Aspirin, Clopidogrel, Simvastatin, Carvedilol, Acyclovir, Finasteride, Calcium acetate, Ranitidine
- Adjunct Pharmacotherapy: Clopidogrel, Bivalirudin
Pre-procedure EKG

Angiograms
Previous
Next
1 of 13
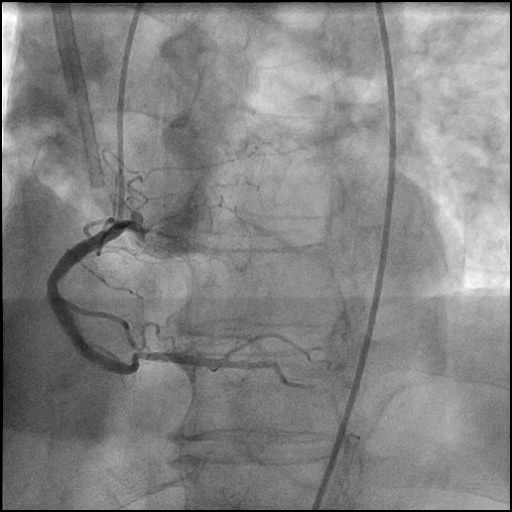
Right coronary artery (RCA) angiography
- 30-50% distal RCA lesion and mild diffuse disease in the right posterior descending artery (RPDA).
1 of 13
Right coronary artery (RCA) angiography 30-50% distal RCA lesion…
2 of 13
Dual injection angiography of the RCA and Left coronary…
3 of 13
Successful wiring across the LAD CTO.
4 of 13
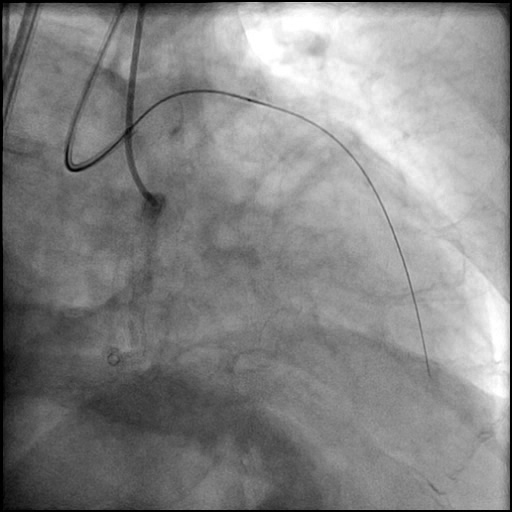
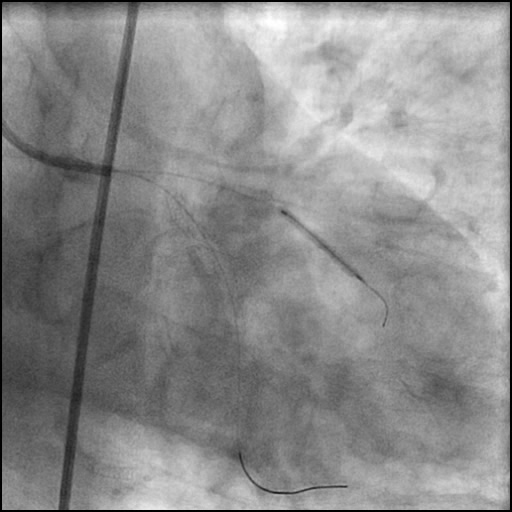
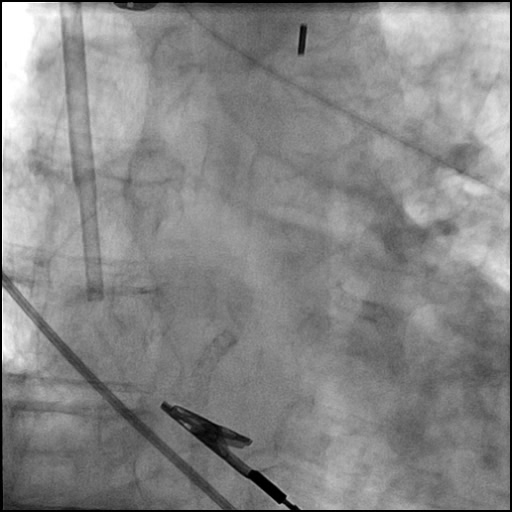
Delivery of a laser atherectomy device to the proximal…
5 of 13
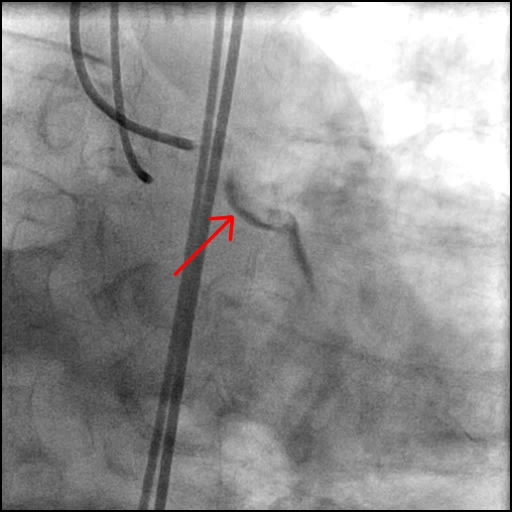
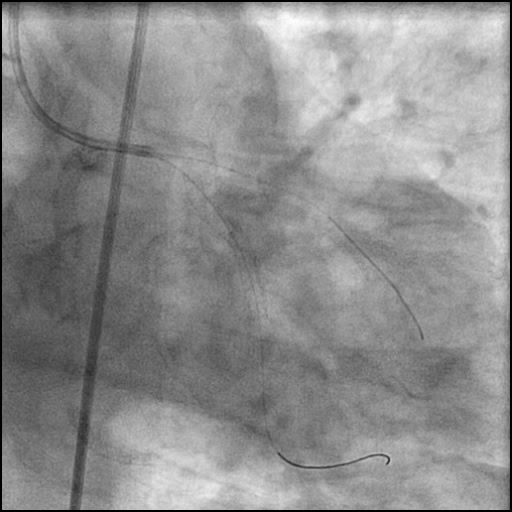
Angiography of the LAD after laser atherectomy showing a…
6 of 13
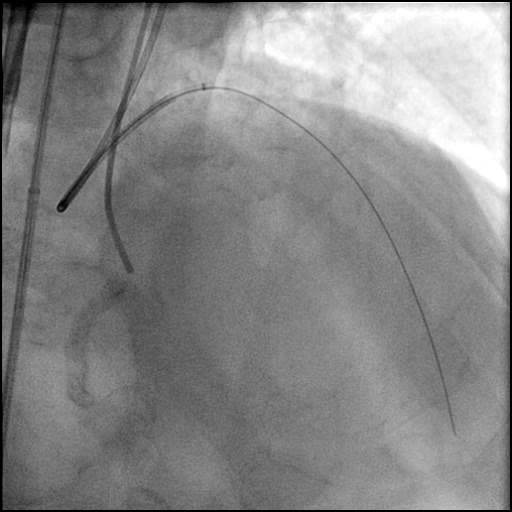
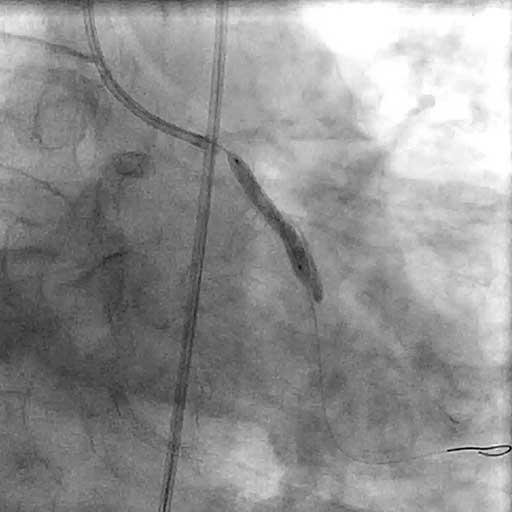
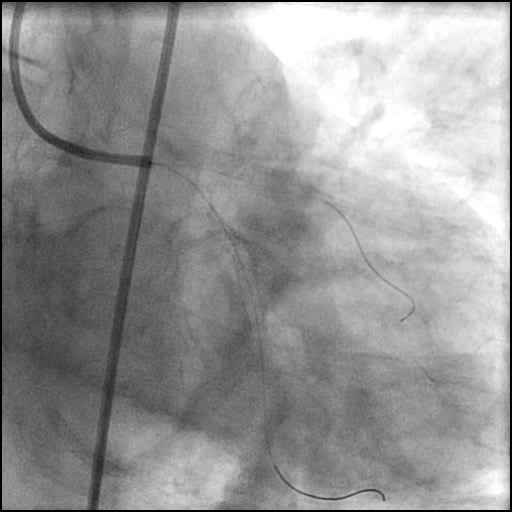
Balloon inflation of the LCx using a NC Quantum…
7 of 13
Angiography of the LCx after balloon inflation showing inadequate…
8 of 13
Angiography after Xience Alpine 3.5/38 mm stent placement in…
9 of 13
Wiring of the RI.
10 of 13
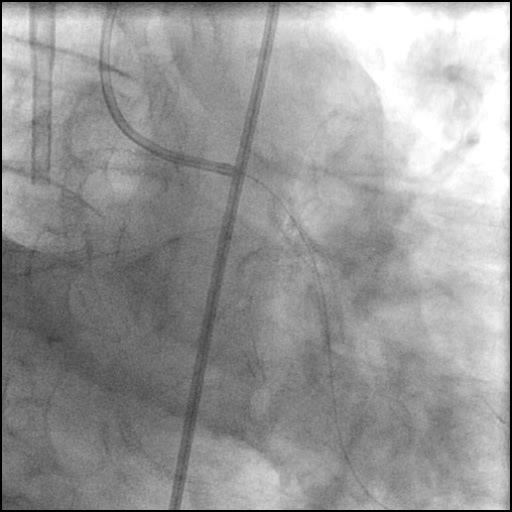
Balloon inflation of the RI using a Trek 2.0/20…
11 of 13
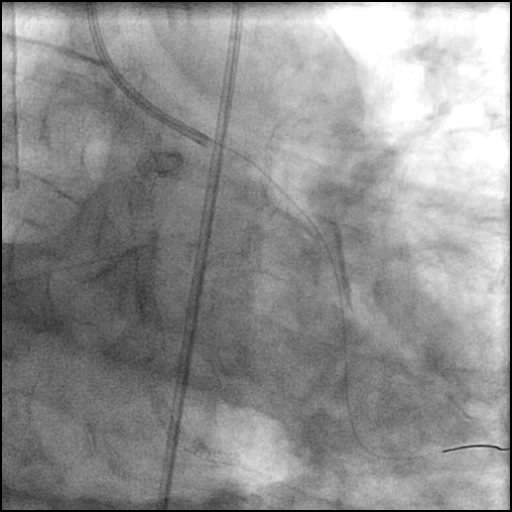
Angiography of the RI after balloon inflation.
12 of 13
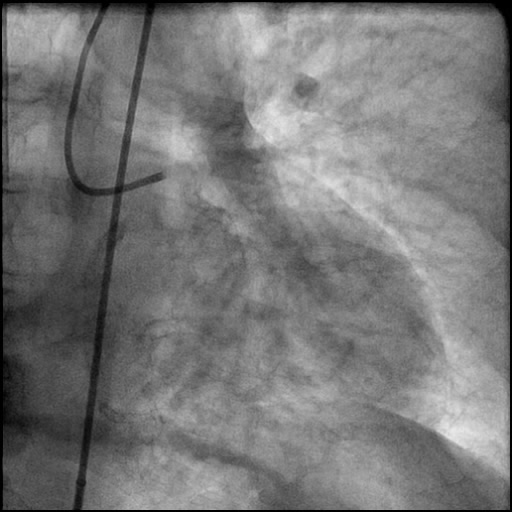
Final angiography showing satisfactory treatment of the LCx and…
13 of 13
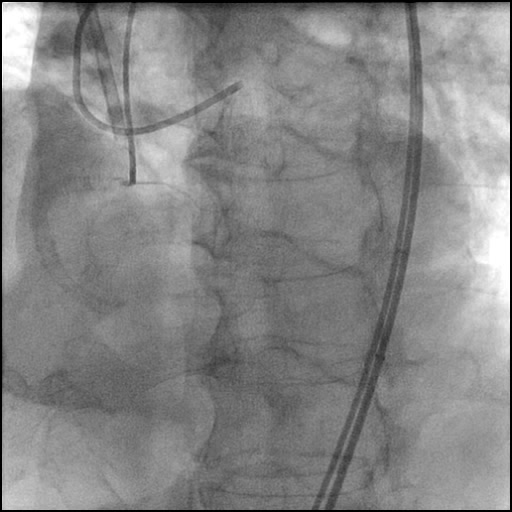
IABP placement.
Post-procedure EKG

Case Overview
- Underwent intervention of the LAD CTO with difficulty delivering equipment across the lesion.
- Laser atherectomy was performed proximal to the LAD CTO with continuous injection of saline through the Guidezilla support catheter.
- Follow up angiography, showed the presence of a flow-limiting Type D dissection of the LCx, and a non-flow-limiting Type D dissection of the RI.
- The proximal LCx dissected segment was promptly treated with balloon inflation followed by successful stent placement.
- The RI dissected segment was treated with serial balloon inflations, stent placement was deferred.
- IABP was placed for hemodynamic support, and intervention to treat the LAD CTO was deferred.
- Echocardiography showed no pericardial effusion.
- Troponin-I peaked at 11.8 ng/mL and CK-MB peaked at 41.0 ng/mL.
- Patient was discharged home two days after the procedure without any sequelae.
Learning Objectives
- What is the likely explanation or reason why the complication occurred?
- Continuous aggressive saline flushing through the Guidezilla support catheter while performing laser atherectomy.
- How could the complication have been prevented?
- Avoid aggressive saline flushing or IC injection of agents (medications, contrast), especially when using a support catheter.
- Continuous saline flushing during laser atherectomy is required and should be performed with low pressure at a rate of 1cc/second.
- Remember to bring back the support catheter back into the guide when performing laser atherectomy.
- Is there an alternate strategy that could have been used to manage the complication?
- Considering the extent of the LCx dissection, direct stenting could have been performed.
- What are the important learning points?
- This is a Type D dissection because of the presence of a spiral filling defect which is clearly outlined with persistence of extraluminal contrast which is present after contrast injection.
- Pay close attention to the entire coronary vascular system when performing a procedure. In this case, the LAD was being intervened on and a dissection involving the LCx and RI occurred.
- In a small to moderate sized vessel with a non-flow-limiting dissection with an optimal angiographic result, after balloon inflation stent placement can be deferred. Hence, we deferred placement of a stent in the RI.
- Given the seriousness and rapid decline in the patient’s hemodynamic status, quick intervention of the LCx and RI was warranted, and further intervention of the LAD CTO was deferred.
- Mechanical hemodynamic support devices should be considered when a patient has hemodynamic compromise.