










Dissection Type D – Case 3
Clinical Presentation
- 56-year-old male who presented with chest pain and found to have a NSTEMI.
Past Medical History
- HLD, Psoriatic Arthritis, Former Tobacco Use, Anxiety
Clinical Variables
- Echocardiography: Inferior, anterior, and anteroseptal wall hypokinesis, LVEF 40-45%.
Medications
- Home Medications: Aspirin, Simvastatin, Sulfasalazine
- Adjunct Pharmacotherapy: Clopidogrel, Bivalirudin
Pre-procedure EKG

Angiograms
Previous
Next
1 of 18
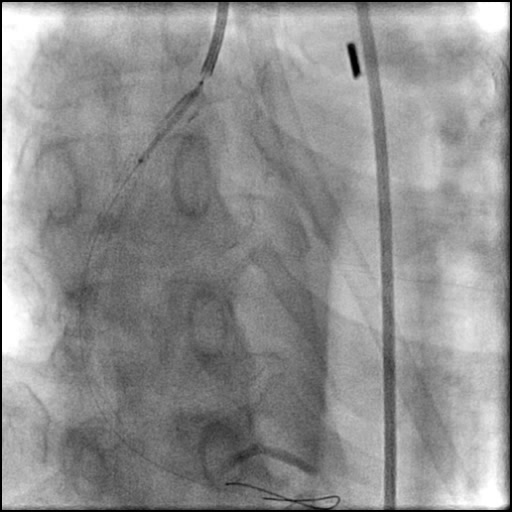
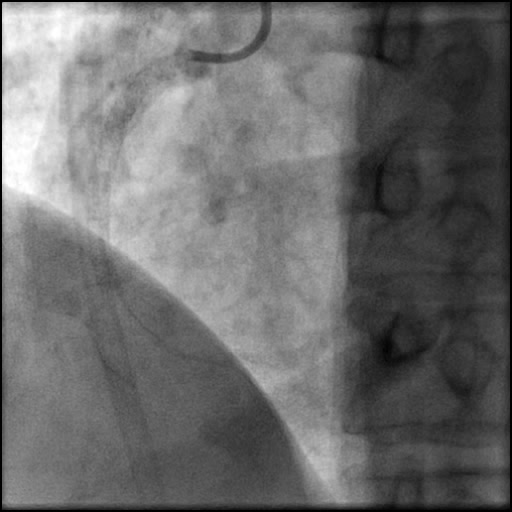
Right coronary artery (RCA) angiography
- 70-80% proximal and 90-95% mid RCA lesion.
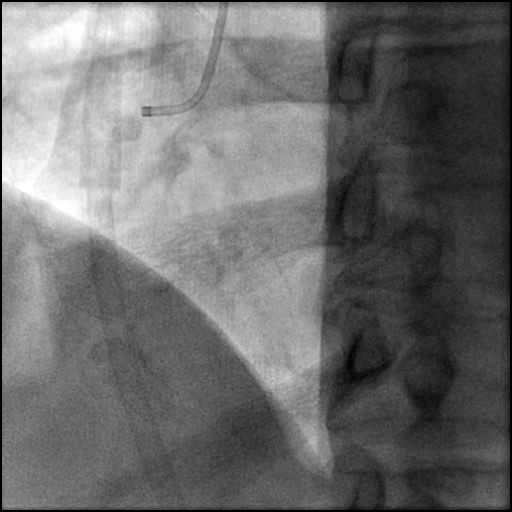
1 of 18
Right coronary artery (RCA) angiography 70-80% proximal and 90-95%…
2 of 18
Left coronary artery (LCA) angiography mild diffuse disease and…

3 of 18
IABP placed, followed by wiring of the LAD.
4 of 18
Positioning of a Xience Xpedition 2.75/28 mm stent in…
5 of 18
Angiography of the LAD after stent placement.
6 of 18
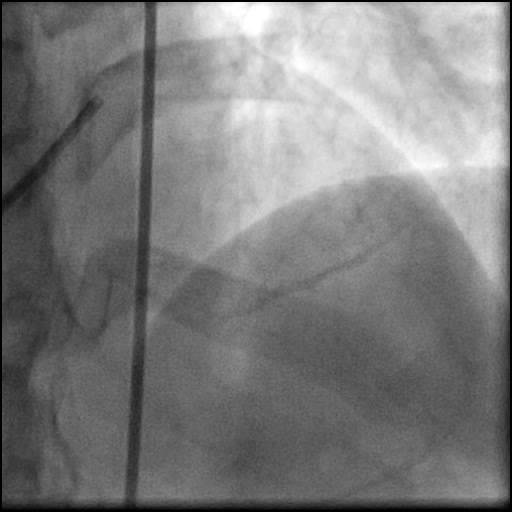
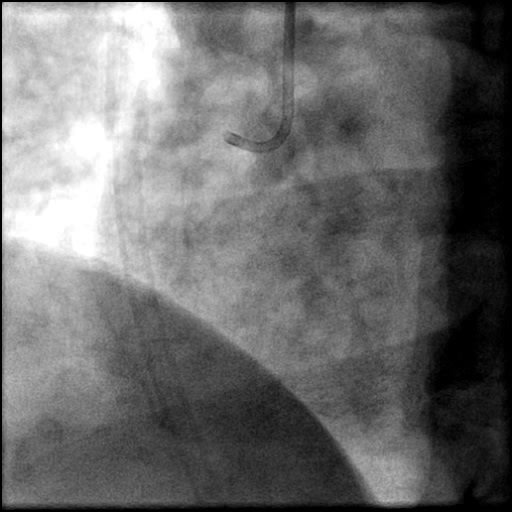
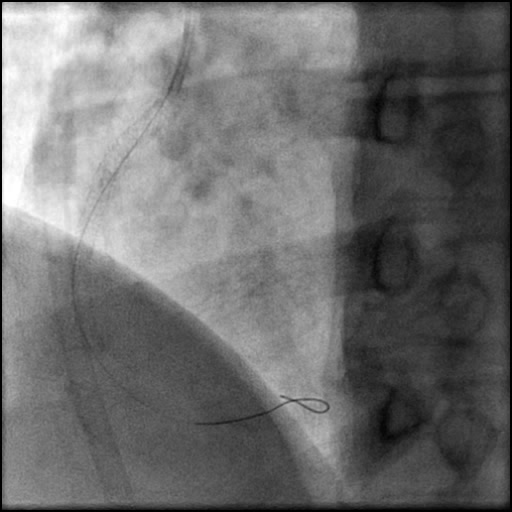
RCA angiography using a guide catheter (IM/6 Fr).
7 of 18
Wiring of the RCA.
8 of 18
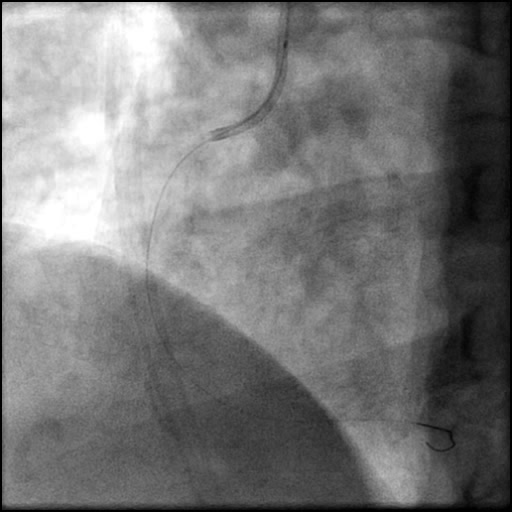
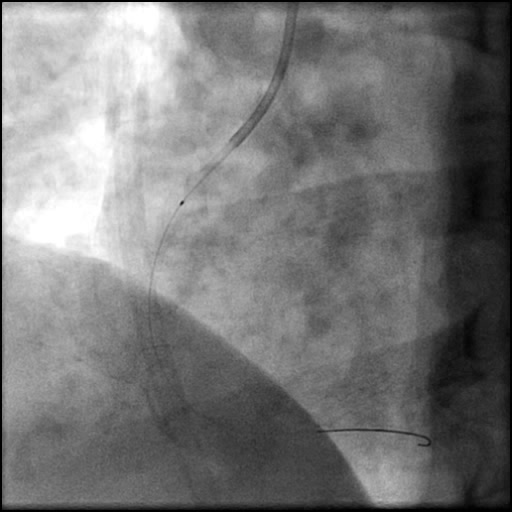
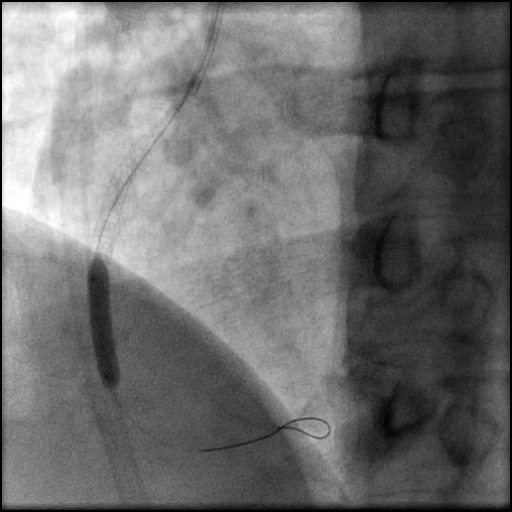
Aspiration thrombectomy of the RCA using an Export Catheter.
9 of 18
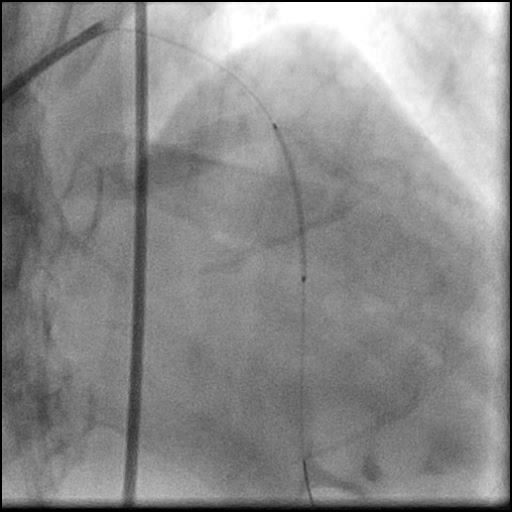
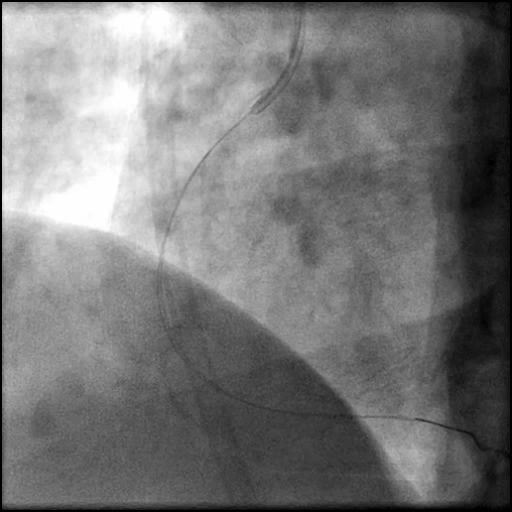
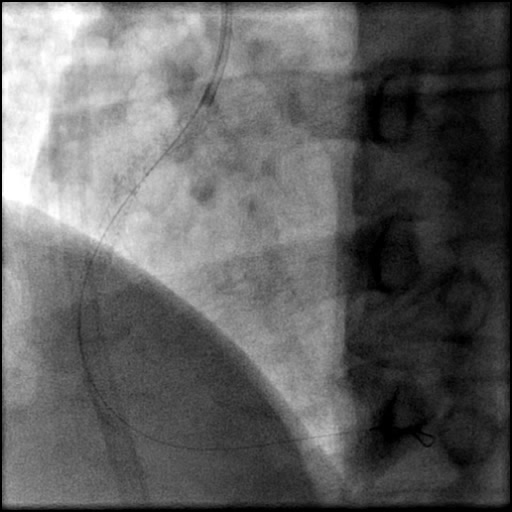
Angiography of the RCA after aspiration thrombectomy showing a…
10 of 18
A second wire was placed in the RCA followed…
11 of 18
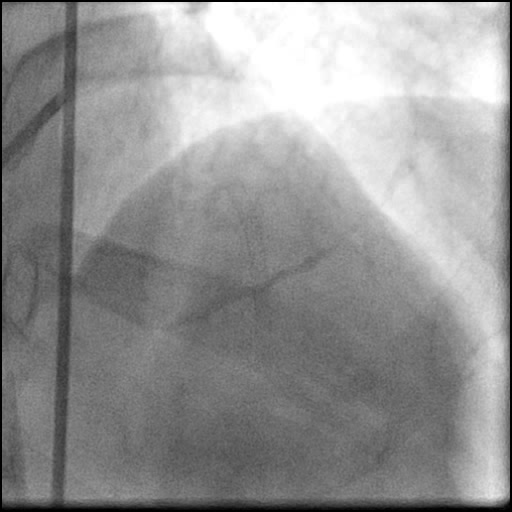
Angiogram of the RCA after balloon inflation showing dissection…
12 of 18
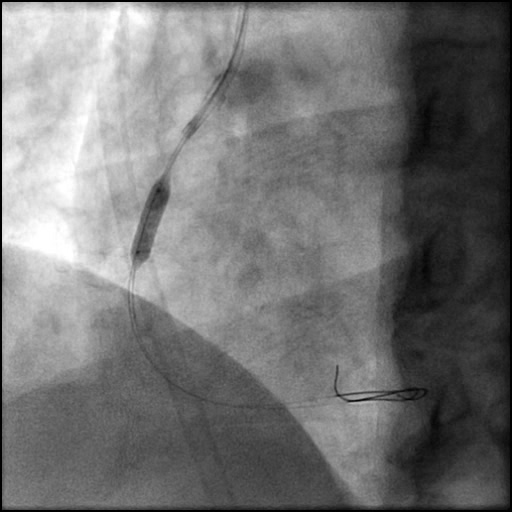
Deployment of a Xience Xpedition 3.5/38 mm stent in…
13 of 18
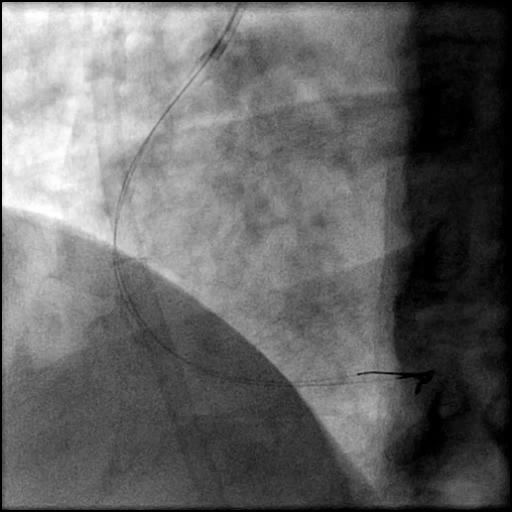
Angiography of the RCA after stent placement.
14 of 18
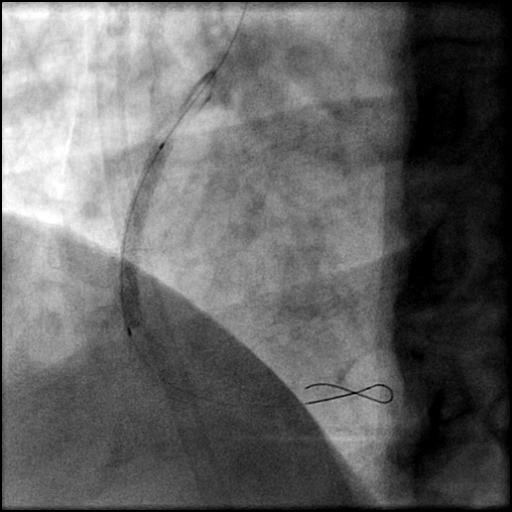
Positioning of a Xience Xpedition 3.5/23 mm stent in…
15 of 18
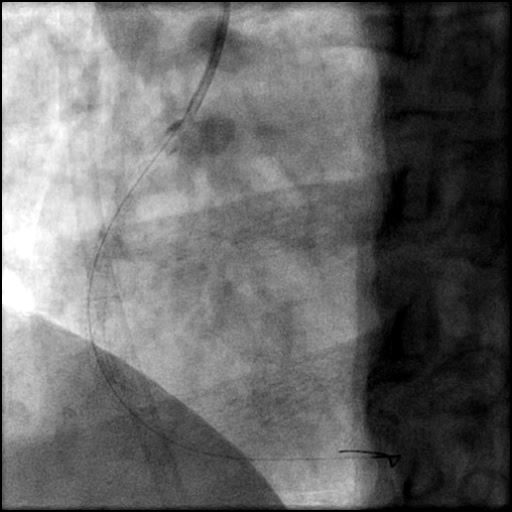
Angiography of the RCA after placement of the second…
16 of 18
Post-dilatation of the stents placed in the RCA with…
17 of 18
Angiography of the RCA after post-dilatation of the stents.
18 of 18
Final angiography showing adequate treatment of the RCA dissection.…
Post-procedure EKG

Case Overview
- Underwent intervention of the LAD and RCA with IABP hemodynamic support.
- LAD intervention was uneventful. This was followed by intervention of the RCA.
- Aspiration thrombectomy of the RCA was performed. Subsequently, a guide catheter (IM/6 Fr) induced, flow-limiting Type D dissection extending from the ostial RCA to the distal bifurcation was noted.
- A buddy wire was positioned for extra support. This was followed by serial balloon inflations and placement of two stents, successfully treating the dissection.
- Echocardiography showed presence of a minimal pericardial effusion with LVEF 40%.
- Troponin-I peaked at 36.4 ng/mL and CK-MB peaked at 36.4 ng/mL.
- Patient was discharged home 5 days later without any sequelae.
Learning Objectives
- What is the likely explanation or reason why the complication occurred?
- Guide catheter-induced injury from aggressive guide catheter handling and manipulation due to the presence of a calcified, severely stenosed RCA lesion.
- Further dissection propagation is due to repeat contrast injections.
- How could the complication have been prevented?
- Maintain guide catheter coaxiality, be cautious with manipulation of the guide catheter, and continuously monitor the position of the guide catheter throughout the procedure. This is extremely important when there is difficulty delivering equipment in tortuous, calcified, long type C lesions.
- Avoid high pressure injections, minimize contrast injection and IC administration of agents (meds, saline) as much as possible.
- Is there an alternate strategy that could have been used to manage the complication?
- Consider stenting the entry/origin of the dissection flap first as this could help prevent further progression of the dissection. However, this strategy may make it more difficult to deliver equipment distally if further intervention is required.
- Stenting of the RCA up to the bifurcation could have been performed, However, during the case wire position was lost and creating uncertainty if the wire was within the true lumen of the RPDA.
- What are the important learning points?
- This is a Type D dissection because of the presence of a spiral filling defect.
- Minimize contrast injection and IC administration of agents (meds, saline) as much as possible, especially when there is a dissection as this can result in dissection propagation.
- Avoid high pressure injections, especially when the catheter is not ideally positioned, or a dissection is present as this can result in dissection propagation.
- Intervention of a complex lesion in a nonculprit vessel should be avoided during STEMI in the setting of cardiogenic shock. In this case, the RCA lesion could have been deferred and intervened on as a staged procedure.