










Dissection Type E – Case 1
Clinical Presentation
- 75-year-old male who presented with chest pain (CCS Class III).
Past Medical History
- HTN, HLD, Hyperlipidemia, CAD s/p PCI, Severe Aortic Stenosis s/p TAVR with 34mm Evolut R CoreValve with mild-moderate paravalvular leak
- LVEF 57%
Clinical Variables
- Prior Cardiac Catheterization: Subtotal RPDA which fills via collaterals from the LAD artery. Underwent unsuccessful PCI of early bifurcating distal RCA-RPDA-AV continuation.
Medications
- Home Medications: Aspirin, Clopidogrel, Atorvastatin, Isosorbide Mononitrate, Olmesartan, Hydrochlorothiazide
- Adjunct Pharmacotherapy: Clopidogrel, Bivalirudin
Pre-procedure EKG

Angiograms
Previous
Next
1 of 13
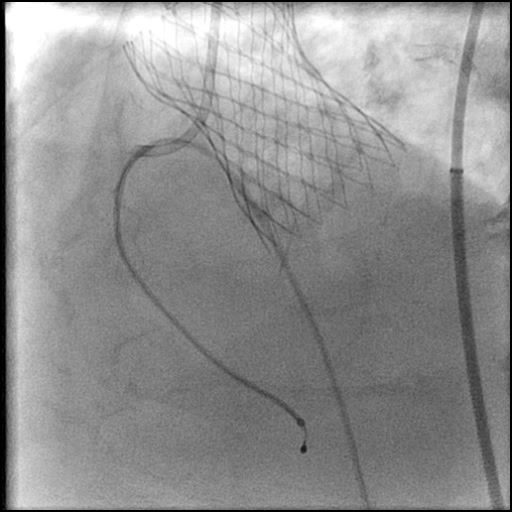
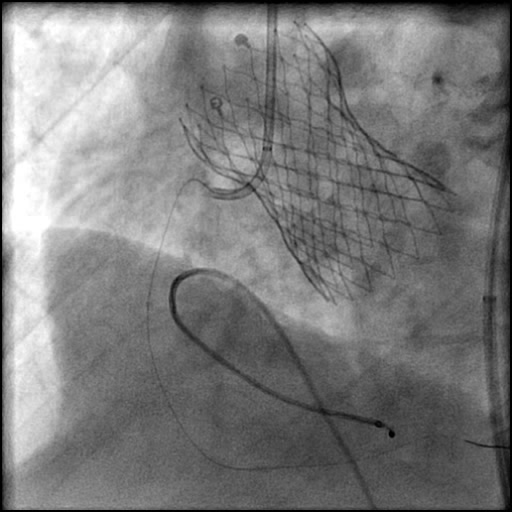
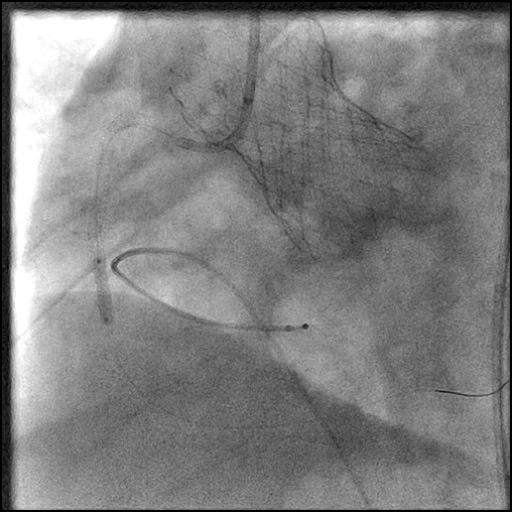
Right coronary artery (RCA) angiography
- 70-80% lesion in the tortuous proximal RCA.
1 of 13
Right coronary artery (RCA) angiography 70-80% lesion in the…
2 of 13
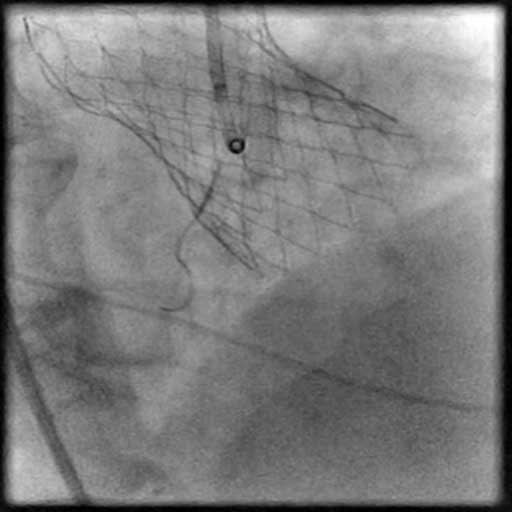
Positioning of a Fielder wire using a Teleport microcatheter.
3 of 13
Pre-dilatation of mid RCA lesion with a Trek 2.5/20…
4 of 13
Pre-dilatation of proximal RCA lesion with a Trek 2.5/20…
5 of 13
Angiography of the RCA after lesion pre-dilatation.
6 of 13
Balloon-assisted tracking performed using a Trek 2.5/20 mm balloon…
7 of 13
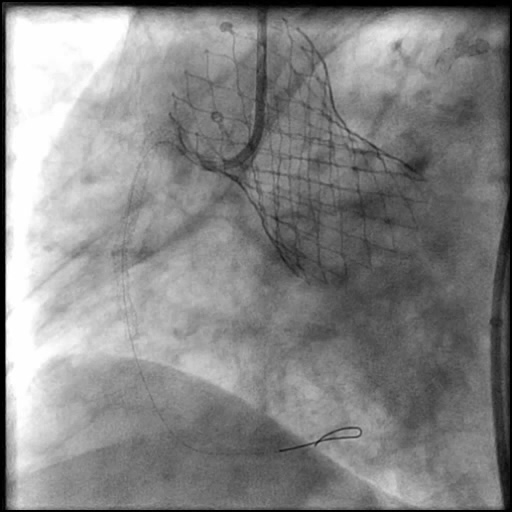
Deployment of a Promus Premier 2.75/38 mm stent in…
8 of 13
Angiography of the RCA after stent placement.

9 of 13
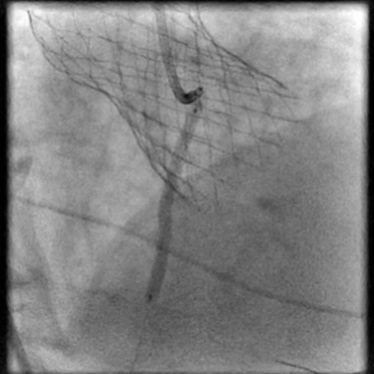
Deployment of a Promus Premier 3.0/12 mm stent in…
10 of 13
Post-dilation of the stents placed in the RCA with…
11 of 13
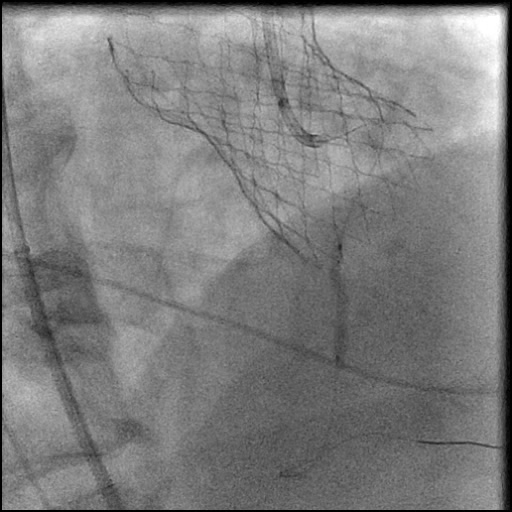
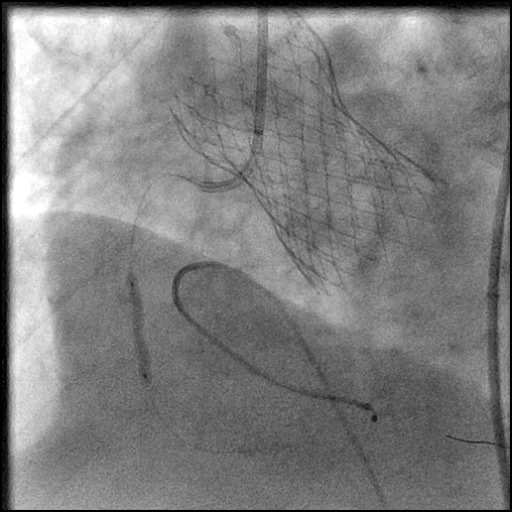
Type E stent edge dissection. IC vasodilators were given…
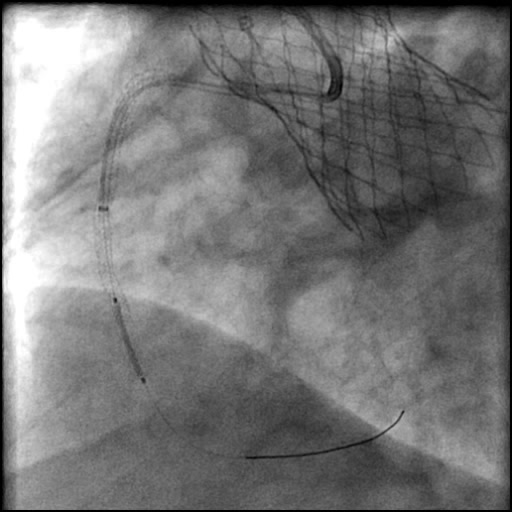
12 of 13
Type E stent edge dissection. IC vasodilators were given…
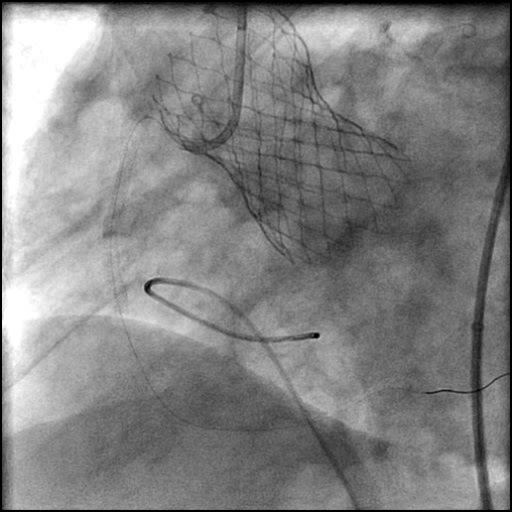
13 of 13
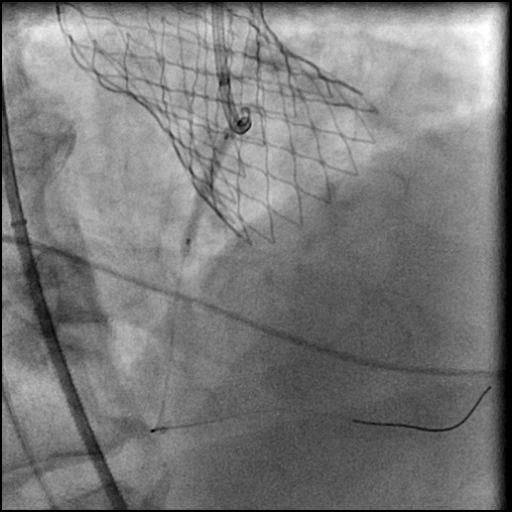
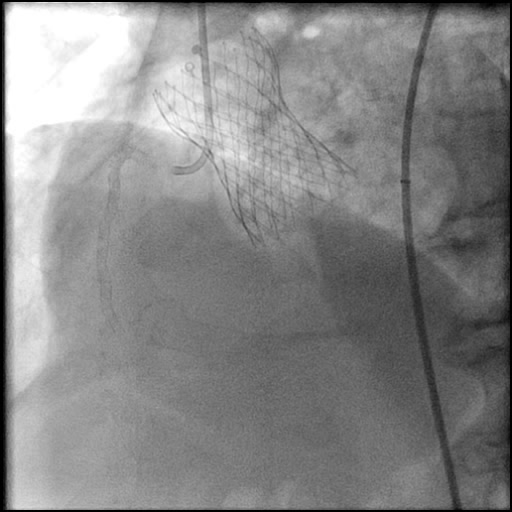
Final angiography showing successful treatment of the RCA dissection.
Post-procedure EKG

Case Overview
- Underwent intervention of the proximal RCA.
- Lesion was pre-dilated followed by placement of a two drug eluting stents.
- Following post-dilatation, procedure was complicated by a minor flow-limiting, Type E distal stent edge dissection.
- IC vasodilators were given with no change in luminal diameter.
- An additional stent was placed, effectively treating the dissection.
- Troponin-I peaked at 0.2 ng/mL and CK-MB peaked at 2.2 ng/mL.
- Discharged home the following day without further sequelae.
Learning Objectives
- What is the likely explanation or reason why the complication occurred?
- High pressure post-dilatation of the distal stent edge.
- How could the complication have been prevented?
- Use lower balloon inflation pressure at the distal stent edge.
- Optimize balloon positioning prior to inflation, assuring the balloon is not outside the stent edge.
- Is there an alternate strategy that could have been used to manage the complication?
- We could have considered performing a prolonged balloon inflation using a NC balloon to tack the dissection flap, then repeat angiography to assess the status of the dissection. and depending on the findings consider placing a stent.
- What are the important learning points?
- This is a Type E dissection because the lumen is enclosed by a flap leading to a persistent filling defect and there is luminal narrowing at the distal stent edge, both which are seen during contrast injection.
- It is important to differentiate between dissection and spasm. When luminal narrowing was noted in the distal stent edge region, we administered IC vasodilators and no change in luminal narrowing was observed, making spasm less likely as the cause of the defect.
- When a stent is placed in a calcified lesion, one needs to be very cautious because there is a higher risk for dissection, particularly along the proximal and distal stent edge.
- Optimize stent post-dilatation technique:
- Use a noncompliant, short balloon for post-dilatation of a stent.
- Keep the balloon just inside the stent edge when performing post-dilatation of the proximal or distal stent edges.
- Use Stent Boost (Philips) or Stent Viz (GE) to assess the positioning of the NC balloon prior to inflation.