










Vasospasm – Case 1
Clinical Presentation
- 73-year-old male who presented with chest pain (CCS Class II).
Past Medical History
- HTN, HLD, DM, CAD s/p 2-Vessel CABG and Multiple PCI’s, Hypothyroidism, CKD
- LVEF 19%
Clinical Variables
- Stress MPI: Mild anteroseptal and posterolateral scarring.
Medications
- Home Medications: Aspirin, Ticagrelor, Carvedilol, Atorvastatin, Isosorbide Mononitrate, Furosemide, Sacubitril-Valsartan, Dulaglutide, Insulin, Levothyroxine, Ranitidine, Allopurinol
- Adjunct Pharmacotherapy: Ticagrelor, Bivalirudin
Pre-procedure EKG

Angiograms
1 of 13
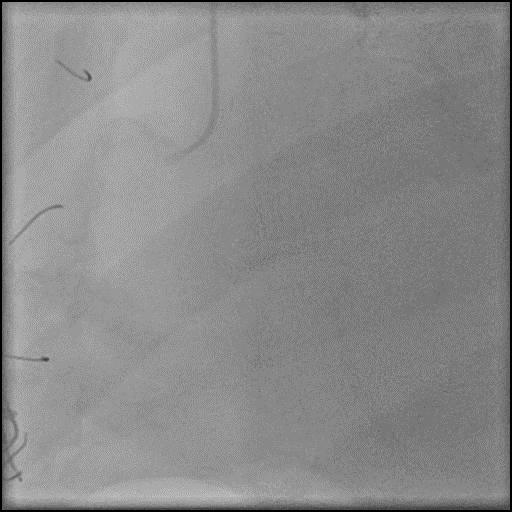
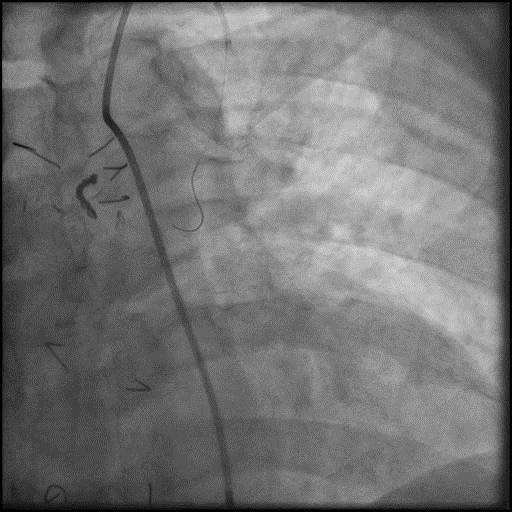
Right coronary artery (RCA) angiography 50-60% distal RCA stenosis
2 of 13
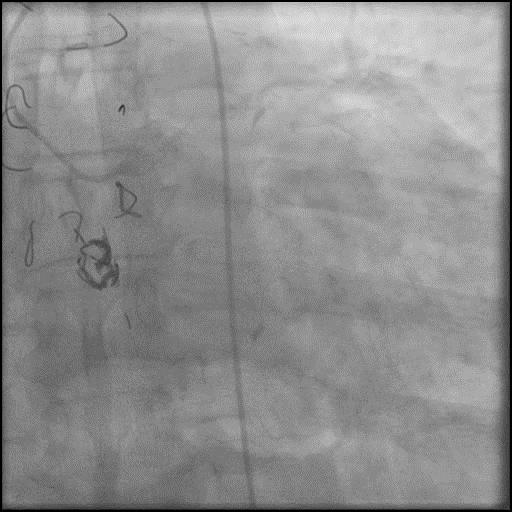
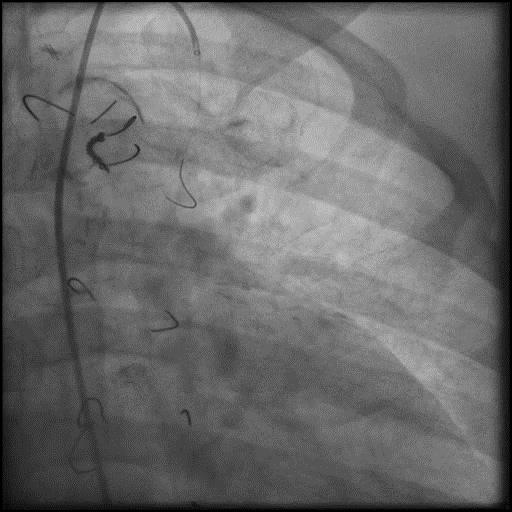
Left coronary artery angiography patent intervention sites in the…
3 of 13
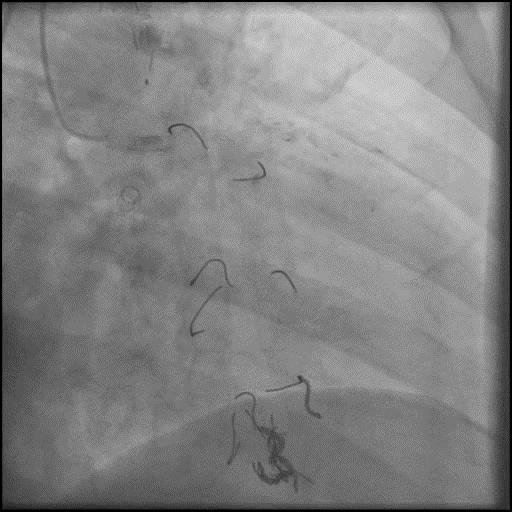
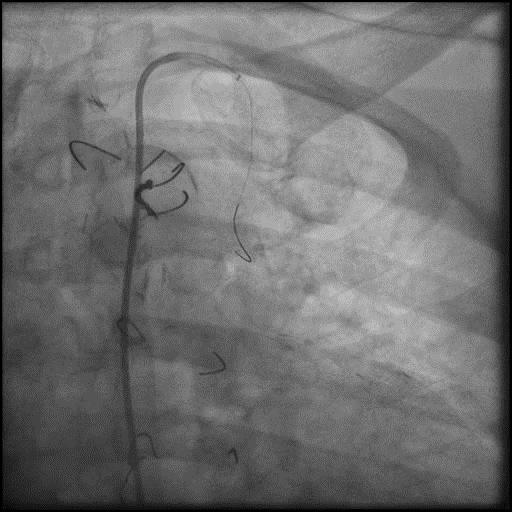
Saphenous vein graft (SVG) to D2 bypass graft angiography…
4 of 13
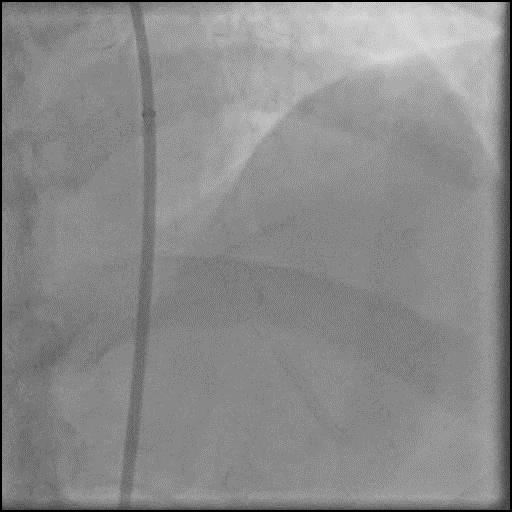
Left internal mammary artery (LIMA) to LAD bypass graft…

5 of 13
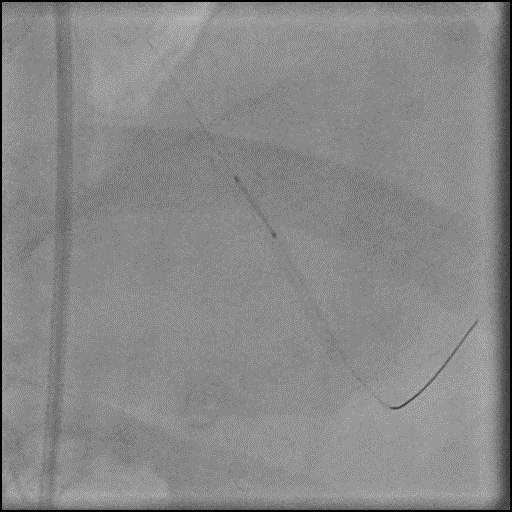
Pre-dilatation of the lesion in the LAD, distal to…

6 of 13
Cutting balloon angioplasty of the lesion in the LAD,…
7 of 13
Positioning of an Xience Sierra 2.75/12mm in the LAD,…
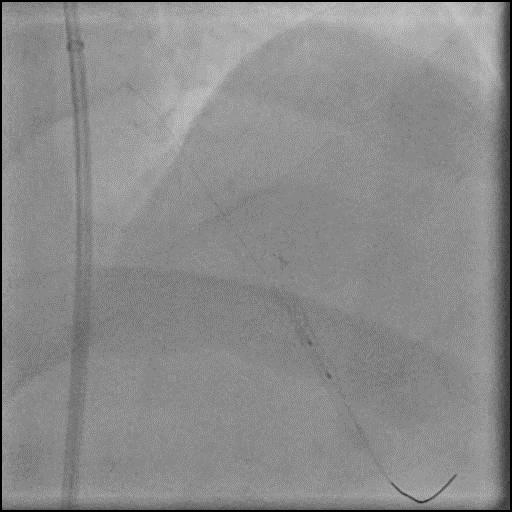
8 of 13
Post-dilatation of the stent placed in the LAD, distal…
9 of 13
Retraction of the wire and the balloon into the…
10 of 13
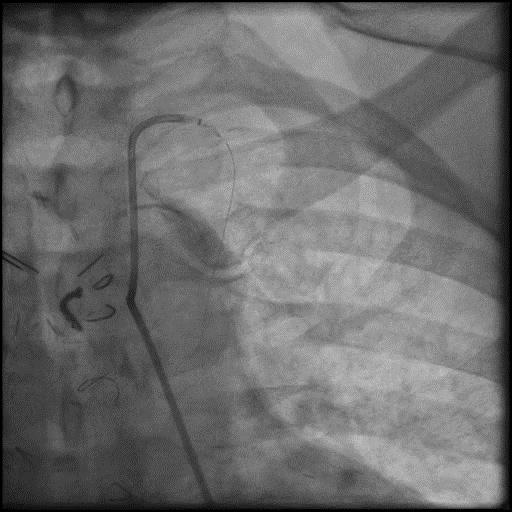
Angiography of the LIMA to LAD bypass graft showing…
11 of 13
The wire was retracted into the proximal LIMA. Angiography…
12 of 13
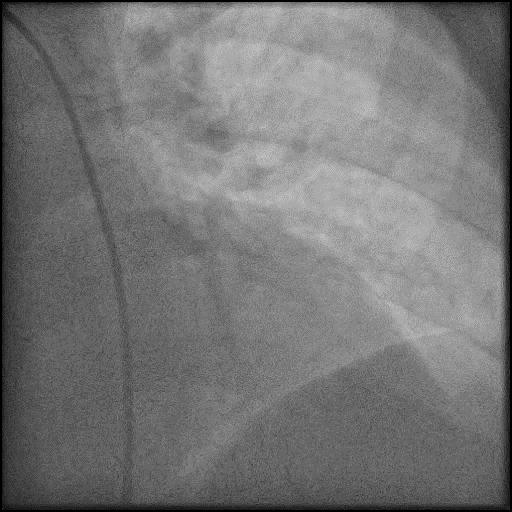
Intra-graft vasodilators were given and majority of the focal…
13 of 13
Final angiography of the LIMA to LAD. The wire…
Post-procedure EKG

Case Overview
- Underwent intervention of the LAD distal to the LIMA to LAD anastomosis.
- After successful intervention of the LAD, the wire and balloon were retracted back into the LIMA.
- Angiography showed presence of multiple focal lesions which were concerning for combined spasm and pseudo-stenosis.
- The wire was further retracted with improvement in some of the lesions distal to the wire; however, many of the focal lesions persisted.
- Intra-graft vasodilators were given and the focal lesions resolved.
- Troponin-I peaked at 0.03 ng/mL and CK-MB peaked at 1.8 ng/mL.
- Patient was discharged home the next day without further sequelae.
Learning Objectives
- What is the likely explanation or reason why the complication occurred?
- Pseudo-stenosis is also known as accordion effect and concertina phenomenon. It occurs when coronary equipment (i.e. coronary guidewire, stent etc.) causes mechanical distortion (folding/pleating) of a coronary artery along its long axis, and it presents as a filling defect.
- Coronary Spasm: the most common cause of intra-procedure coronary spasm is guidewire or balloon/stent manipulation. Catheter-induced spasm which usually involves the RCA ostium more often than the LCA ostium, and typically is within 2cm of the catheter tip. Cases where rotational atherectomy is used are more prone to coronary spasm. Coronary spasm occurs because of endothelial denudation and nitric oxide loss.
- How could the complication have been prevented?
- Use a less supportive/stiff coronary guidewire.
- Vasodilators should be given prophylactically and for treatment of coronary spasm, especially when performing ostial RCA and LCA interventions.
- Is there an alternate strategy that could have been used to manage the complication?
- It is reasonable and safer to diagnose pseudo-stenosis while leaving a guidewire within the coronary artery, and withdrawing it gradually until its radio-opaque (floppy) segment rests equally on either side of the suspect lesion. However, this technique is usually not feasible when there are multiple discreet lesions. If this technique fails, focal defect is located in the distal segment of a large vessel, reduced coronary flow with ongoing chest pain and EKG changes, or if there are multiple discreet lesions, then use a transit exchange catheter to remove the coronary guidewire. Place the exchange catheter distally over the guidewire and the remove the guidewire. This usually allows the vessel to return to its natural contour, resolving the pseudo-stenosis. It is important to position the exchange catheter distal as possible before removing the coronary guidewire because once the wire is removed, the vessel tortuosity will be restored and some position will be lost when reintroducing the wire. The guidewire can be exchanged, for a less supportive wire that will better conform to the artery contour if needed.
- Step by step algorithm for management of coronary spasm:
- 1st: Intra-coronary/intra-graft vasodilators should be given slowly through a catheter, especially if using a guide catheter with side holes to maximize delivery into the artery. If one agent is unsuccessful, give combined therapy as CCB and nitrates have additive effect. We use the following agents and administer them intra-coronary/intra-graft:
- Nitroglycerin 100-200 mcg, Verapamil 100-200 mcg, Nicardipine 100-200 mcg
- 2nd: If medical therapy fails, remove hardware without losing coronary guidewire position to minimize mechanical provocation.
- 3rd: If persists, consider performing prolonged (2-5 min) PTCA at low pressure (1-4 atm).
- 4th: In rare cases, a stent can be placed if above measures fail. Placement of a stent should be avoided as much as possible because it may propagate the spasm in either direction of the stent. Remember, refractory spasm may be indicative of dissection, which is also treated with a stent.
- Intra-coronary/intra-graft imaging with IVUS/OCT may be used to help elucidate the etiology of a focal lesion.
- What are the important learning points?
- If a new lesion appears while performing a procedure an operator has to consider a broad differential which includes coronary spasm, thrombus, dissection, plaque shift, and pseudo-stenosis.
- Coronary spasm is classified as:
- Focal coronary spasm : involves a single localized segment of a single coronary artery
- Multifocal coronary spasm: involves multiple localized segments of the same coronary artery
- Multivessel coronary spasm: involves segment(s) of more than one coronary artery
- Coronary spasm may appear benign but can lead to life-threatening arrhythmias and conduction abnormalities. Prognosis is worse in patients who have combined CAD and coronary spasm.
- Definitive diagnosis of coronary spasm is made angiographically when there is a luminal narrowing in a segment of a vessel that is shown to be reversible, typically with administration of intracoronary vasodilators.
- If there is a new focal lesion after introduction of coronary equipment, remember to review the initial acquisitions and follow the algorithm above. Often times both a spasm and pseudo-stenosis can present simultaneously, and both IC vasodilators and removal of coronary equipment is necessary for the filling defect to resolve. However, if there is concern for dissection or thrombus, wire position should NOT be lost.