










- Home
- ComplicAID Home
- Miscellaneous Book
DEVICE EMBOLIZATION
- Device embolization is a rare PCI complication defined as a loss of a device such as stent, guidewire, catheter fragments or misplaced intravascular coils within the coronary vasculature
- Incidence: Stents are the most common devices embolized, with an incidence ranging from 3% for the first-generation hand-crimped devices to much lower, 0.32%, for current stent delivery system1
- Risk factors:2
- Extreme tortuosity
- Angulation
- Calcified vessels
- Inadequate guide catheter support
- Older generation stents
- Device dislodgement may result in systemic or intracoronary embolization. While systemic embolization may cause severe cerebro-
vascular events, limb ischemia, death and the need for an emergency surgery, intracoronary embolization is associated with high risk of coronary thrombosis and subsequent MI3
- A tortuous and calcified coronary anatomy increases the rigidity of the vessel making it prone to a stent peeling off the balloon as increased force is applied to advance the device. For this reason, stents are more commonly lost in the right coronary and left circumflex arteries and less commonly in the left anterior descending artery4
- Prevention: When facing difficulty delivering a stent:
- Stop and gently retract stent back into the guide catheter and remove it instead of forcing it forward
- Perform pre-dilatation of the lesion if a direct stenting was attempted or if lesion
was predilated perform further dilation using higher atmospheric pressure or bigger balloon or use atheroablative devices for adequate lesion preparation
- Make sure the tip of guide is coaxial especially if there is significant proximal tortuosity
- Use of guide extension catheters can help deliver the stents
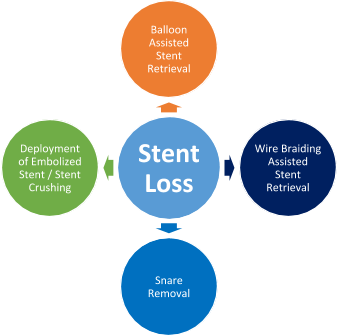
- Management - These are the key steps for managing device embolization during PCI:
- If embolized item is a small guidewire, consider leaving wire in the coronary artery
- No treatment is required for peripherally embolized small stents
- Consider surgical removal if involves larger coronary arteries or difficult vascular access sites or if all the techniques fail to retrieve the device
- Balloon assisted stent retrieval: After withdrawal of the stent balloon from which the stent has become dislodged, a second smaller 1.5 or 2 mm balloon is advanced over the wire and through the stent, and is inflated distal to the stent. Then it is retracted back into the guide. In some cases, the stent may be contained within the distal tip of the guide, but the inflated balloon cannot be retracted into the guide. In this scenario, the guide and balloon should be removed as one unit over the wire. Two balloons are required if the stent diameter is too large for a single balloon to retract.
- Snare removal - This is the most widely used tool for stent retrieval. Many snares are available commercially; gooseneck snare is most commonly used. Once a stent slips off the delivery balloon, the
indwelling wire is advanced as far as possible into the distal vasculature. The loop of the snare is passed over the angioplasty wire, encircles it, and is advanced up to the coronary ostium. It arrives at the right position as its loop is encircling the proximal end of the stent. The loop is tightened by advancing the transport catheter, and the whole stent–snare–wire complex is withdrawn as a unit.
- Wire braiding assisted stent retrieval: - This method is useful if the stent has come off the balloon but remains on the wire. A second, soft-tipped wire is navigated strategically through the side struts and not the central lumen. It is then passed into a branch distal to the stent and is separate from the first wire.
Torque is then applied to both wires, and the twisting action results in them wrapping around both sides of the stent, trapping the stent in between. With gentle and persistent pulling, the whole system (guide, stent twisted between two wires) can be withdrawn. An extension catheter can be used to help retrieve the stent.
- Deployment of embolized stent/Stent crushing or stent exclusion: If attempts for retrieval are unsuccessful, it may be necessary to consider stent crushing to the arterial wall with balloon inflation or deployment of an additional stent alongside the embolized one, although this is associated with an elevated risk of periprocedural MI, death, and referral for CABG. Even if the stent is not advanced
completely through the lesion, it should be expanded where it is to its fullest possible dimension using the deployment balloon. If the deployment balloon cannot be advanced through the stent, a balloon with a lower profile should be inserted.
OSTIAL PCI COMPLICATION
- Percutaneous intervention of ostial lesions in coronary arteries or aortocoronary bypass grafts can pose unique challenges and is associated with higher procedural and medium-term complication rates.5
- Ostial lesion is defined as one arising within 3 mm of the vessel origin. It may be categorized by location as- Aorto-ostial, non aorto-ostial and branch ostial.6
- In the balloon angioplasty era, procedural complications such as dissections, acute vessel closure and myocardial infarction were more frequent.7 This led to interest in the use of adjunctive devices such as directional atherectomy, rotational atherectomy, excimer laser and cutting balloons for the purposes of debulking or modifying plaque at ostial sites, with varying degrees of success. With the
introduction of bare metal stents and drug eluting stents, the restenosis rates and complication rates reduced as compared to balloon angioplasty but the outcomes of placement of DES at ostium still remain inferior to non-ostial lesions.8, 9
- Iatrogenic aortocoronary dissection complicating coronary interventions is extremely rare and a few cases have been reported. The incidence of this complication is approximately 0.02% for diagnostic coronary angiography and 0.02-0.83% for PCI procedures.10
- The rapid propagation of aortocoronary dissection may become life threatening and should be recognized immediately. Most reported iatrogenic aortocoronary dissections have been related to procedures in the RCA, especially during PCI for chronic total occlusions.11
- These are some of the unique complications of ostial PCI:
- The calcified ostium may lead to incomplete stent expansion and predispose to restenosis or stent thrombosis
- Direct contact between the guiding catheter and the proximal edge stent struts may lead to longitudinal stent deformation
- Trauma to the ostium from the guide catheter or during balloon inflation may result in dissection of the coronary artery and aortic root
- There are higher chances of stent misplacement and excessive stent protrusion
Prevention and Treatment of Ostial PCI complications
Guide catheter-induced dissection/occlusion of flow- Selection of less aggressive guide catheters
- Cautious catheter manipulation
- Rapid wiring and pre-loading coronary wire before guide engagement
- Once wire down the vessel try and disengage the guide from ostium to avoid ostial occlusion in case of tight ostial lesions
- Anticlockwise rotation to disengage catheter from RCA ostium
- Aorto-coronary dissection can be successfully managed by stenting of the entry point of the coronary dissection if the dissection extends 40 mm from the ostium or in cases of occlusion of the dissected vessel with cessation of antegrade flow that cannot
be restored percutaneously, and if the extension of the dissection is up to the descending aorta12
Misplacement of the stent- Optimal angiographic views with proximal positioning of stent marker
- The stent should be positioned protruding into the aorta by 1–2 mm to prevent recoil of the lesion at the stent edge
- Avoid using very short (<12 mm) stents to ensure adequate anchoring of the stent and to provide adequate lesion coverage distally
- Use the presence of ostial calcium to assist with stent positioning
- Stent pull-back technique for non aorto-ostial sites13
- Make sure to prepare lesion adequately, use of cutting balloon, rotational atherectomy is highly recommended
- Routine use of high pressure non-compliant balloon for post dilation
- Use of IVUS to assess for stent sizing and expansion is recommended
- Accurate stent positioning crucial
- If risk of side branch closure high (calcified, pre-existing lesion >50%, tortuous. lesion length >10mm) consider wire protection or upfront dedicated 2 stent bifurcation stenting if side branch size >2.5mm14
- Kissing PTCA to side branch if flow compromised
- IC vasodilators to exclude spasm
- Avoid deep intubation with guiding catheters or extension systems through already stented segment
- If resistance to passage of a secondary device in the stent do not push hard
- When LSD is suspected, radiographic assessment of the stented segment, preferably with StentBoost (Philips, Andover, Massachusetts) or an equivalent image-enhancement program, should be done
- Confirm wire position and use a small compliant balloon followed by a high-pressure noncompliant balloon aiming to ensure adequate expansion of deformed
stent struts and their apposition to coronary arterial. If LSD still persists, another stent can be used
- IVUS is strongly encouraged, although it is advisable to proceed to intracoronary imaging once LSD has been treated to avoid further potential deformation
- Adequate lesion preparation to prevent stent crossing failure
- Optimal angiographic views to accurately position the proximal stent marker
- Since the guide is disengaged during stent positioning, it may be difficult to visualize the ostia. If possible, use the presence of ostial calcium to assist with stent positioning
- Stent pull-back technique for non aorto-ostial sites13
- Use of buddy wire for positioning marker in side branch or aorta
- After stent deployment, perform light “flaring” of the ostium of the stent
- Use of Flash Ostial Balloon may be used for flaring of ostial stent15
- Adequate lesion preparation is key
- Avoid stent edge deployment at site of significant plaque (Imaging helpful)
- In case of dissection or perforation use prolonged balloon inflation +/- another stent deployment
References
- Brilakis E.S., Best P.J.M., Elesber A.A., et al. (2005) Incidence, retrieval methods, and outcomes of stent loss during percutaneous coronary intervention. Catheter Cardiovasc Interv 65:333–340.
- Bolte J., Neumann U., Pfafferott C., et al. (2001) Incidence, management, and outcome of stent loss during intracoronary stenting. Am J Cardiol 88:565–567.
- Kozman H., Wiseman A.H., Cook J.R. (2001) Long-term outcome following coronary stent embolization or misdeployment. Am J Cardiol 88:630–634.
- Francesco Giannini, Luciano Candilio, Satoru Mitomo, Neil Ruparelia, Alaide Chieffo, Luca Baldetti, Francesco Ponticelli, Azeem Latib, Antonio Colombo. Practical Approach to the Management of Complications During Percutaneous Coronary Intervention. J Am Coll Cardiol Intv. 2018 Sep, 11 (18) 1797-1810.
- Tan KH, Sulke N, Taub N, Sowton E. Percutaneous transluminal coronary angioplasty of aorta ostial, non-aorta ostial, and branch ostial stenoses: acute and long-term outcome. Eur Heart J 1995;16:631-9.
- Mavromatis K, Ghazzal Z, Veledar E, Diamandopoulos L, Weintraub WS, Douglas JS, Kalynych AM. Comparison of outcomes of percutaneous coronary intervention of ostial versus nonostial narrowing of the major epicardial coronary arteries. Am J Cardiol 2004;94:583-7.
- Jokhi P, Curzen N. Percutaneous coronary intervention of ostial lesions. EuroIntervention 2009;5:511-514.
- Rocha-Singh K, Morris N, Wong SC, Schatz RA, Teirstein PS. Coronary stenting for treatment of ostial stenoses of native coronary arteries or aortocoronary saphenous venous grafts. Am J Cardiol 1995;75:26-9.
- Iakovou I, Ge L, Michev I, Sangiorgi GM, Montorfano M, Airoldi F, Chieffo A, Stankovic G, Vitrella G, Carlino M, Corvaja N, Briguori C, Colombo A. Clinical and angiographic outcome after sirolimus-eluting stent implantation in aorto-ostial lesions. J Am Coll Cardiol 2004;44:967-71.
- Dunning DW, Kahn JK, Hawkins ET, O'Neill WW. Iatrogenic coronary artery dissections extending into and involving the aortic root. Catheter Cardiovasc Interv. 2000;51(4):387–393.
- Boukhris M, Tomasello SD, Marzà F, Azzarelli S, Galassi AR. Iatrogenic aortic dissection complicating percutaneous coronary intervention for chronic total occlusion. Can J Cardiol. 2015;31(3):320–327.
- Wykrzykowska JJ, Ligthart J, Lopez NG, Schultz C, Garcia-Garcia H, Serruys PW. How should I treat an iatrogenic aortic dissection as a complication of complex PCI? EuroIntervention. 2012;7(9):1111–1117.
- Kini AS, Moreno PR, Steinheimer AM, et al. Effectiveness of the stent pull-back technique for nonaorto ostial coronary narrowings. Am J Cardiol. 2005;96(8):1123-1128. doi:10.1016/j.amjcard.2005.06.043.
- Sharma SK, Sweeny J, Kini AS. Coronary bifurcation lesions: a current update. Cardiol Clin. 2010;28(1):55‐70. doi:10.1016/j.ccl.2009.10.001.
- Riley R, Lombardi B. Solving the dilemma of ostial stenting: a case series illustrating the flash ostial system.Cardiol Cardiovascmed. 2017;1(1):64-71.
