










Angiographic Haziness Caused by Heavy Calcification
A 55-year old male with a history of controlled hypertension, hyperlipidemia, and positive stress test presented with atypical chest pain. Coronary angiography showed a hazy filling defect in the left anterior descending (LAD) coronary artery (Figure 1, A, B, arrows).
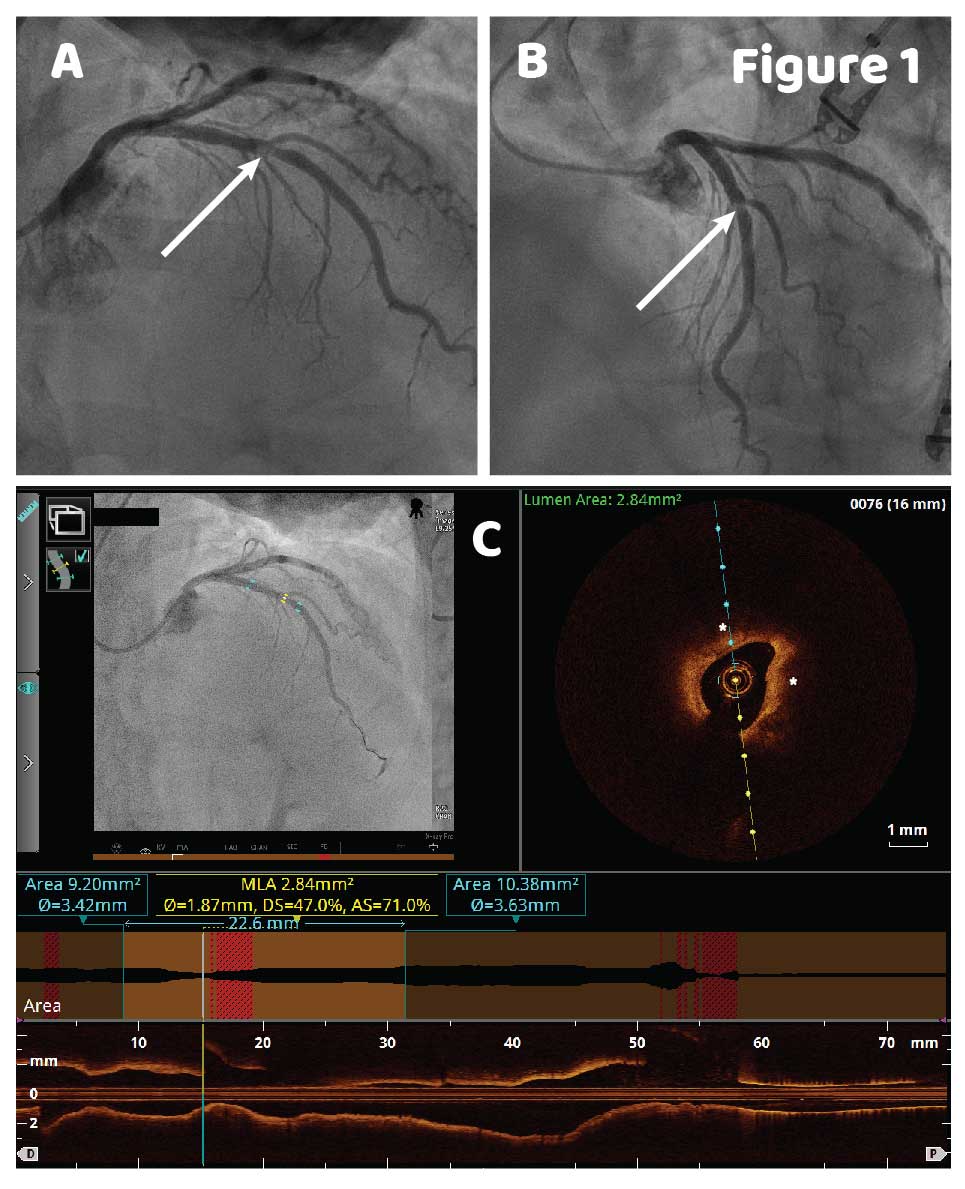
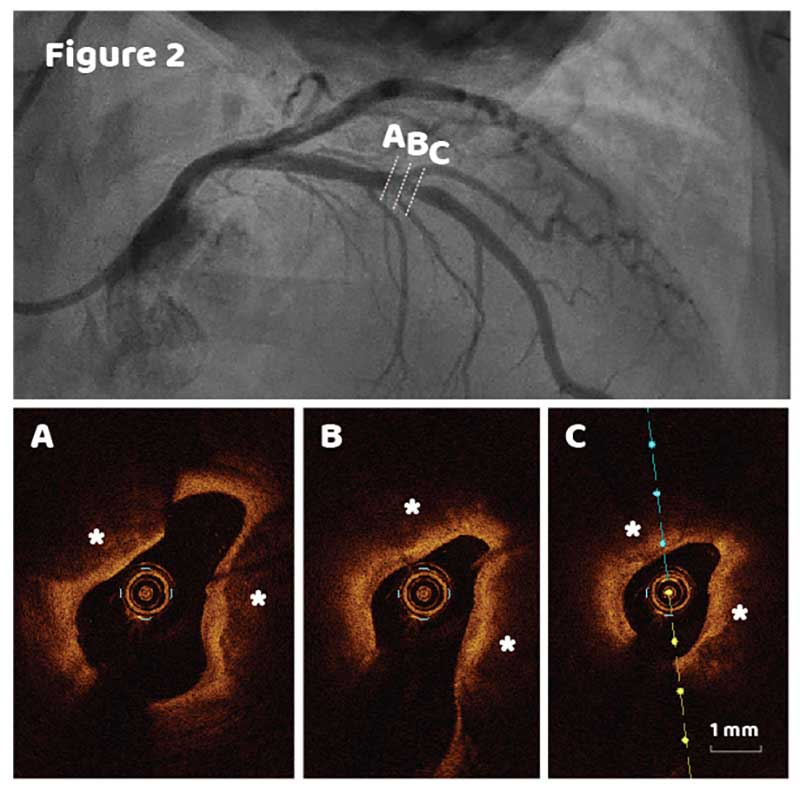
OCT imaging co-registered with angiography was performed to further assess the LAD (Figure 1C). At the site of the filling defect (yellow markers in angiography image in C) fibrocalcific lesion with > 180o of calcium was detected by OCT. Several OCT frames representing angiographic “hazy” area shown in Figure 2 demonstrate severely calcified plaque without any signs of intraluminal thrombus. Non-circular lumen shape and calcific deposit locations (marked by asterisks, located across each other) might be responsible for the angiography haziness.
Lesion minimal lumen area was 2.84mm2 and area stenosis 71% (Figure 1C, automatic measurements shown in the lumen profile window above the longitudinal view). Distal and proximal reference diameters were 3.42mm and 3.63mm, lesion length 22.6mm. Based on OCT lesion morphology characteristics and quantitative assessment, calcified bifurcation lesion was treated by rotational atherectomy with 1.75mm burr followed by a drug eluting stent implantation (3.5mm X 18mm) using provisional stenting technique with final kissing balloon inflation (KBI) performed due to the side branch ostial pinch. Post-stent result was verified using additional OCT pullback, which confirmed good stent apposition and expansion with minimal stent area 6.1mm2 and percent area stenosis 81.3% (Figure 3).

Angiographic “haziness” is considered a sign of a complicated lesion and is usually represented by an angiogram with nonhomogeneous contrast density, indistinct borders or “ground glass” appearance. In this case, OCT helped identify the cause of a hazy filling defect on coronary angiography. An intracoronary thrombus and heavy calcification might have identical angiographic appearance, but require different treatment approaches (1). A heavily calcified lesion might be suitable for atherectomy, which would be a contraindication for a lesion with large thrombus.
References
1 Kini AS. Coronary angiography, lesion classification and severity assessment. Cardiol Clin. 2006 May; 24(2):153-62
1 Kini AS. Coronary angiography, lesion classification and severity assessment. Cardiol Clin. 2006 May; 24(2):153-62
Ask the Experts

Ask the Experts
We are ready to help you.
ask now
ask now
Take Quiz

Take Quiz
Know about OCT? Test your knowledge.
try it now
try it now
Meet the Team

Meet the Team
Read about the team behind the apps.
learn more
learn more
Contact Us

Contact Us
Reach out to us with general comments or questions.
connect now
connect now