










OCT Guidance in Bifurcation PCI of Proximal LCx and LAD
A 65-year-old male, with a history of hyperlipidemia and prior PCI to RCA and LAD, presented with NSTEMI. Coronary angiography revealed three vessel disease and the patient underwent successful intervention of culprit RCA lesion with rotational atherectomy and DES implantation. Subsequent stress MPI revealed moderate to severe lateral, infero-lateral and mild apical ischemia. Angiography showed 70% proximal LAD in-stent restenosis lesion and 90% multiple calcified lesions in the LCx (Figure 1).

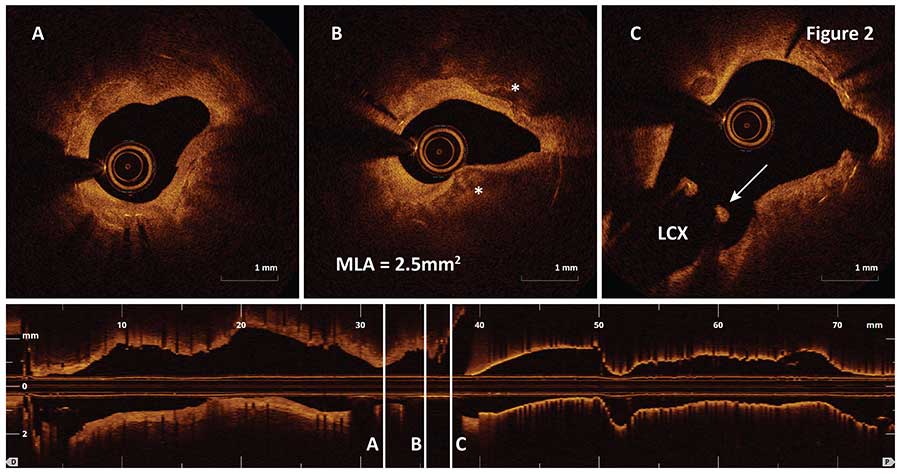
OCT pullback performed in the LAD using a fast survey mode detected a single stent layer with mostly fibrous intimal hyperplasia (Figure 2A), fibrocalcific plaque around the MLA site (Figure 2B, asterisks) and stent struts overlaying the LCx (Figure 2C, arrow).
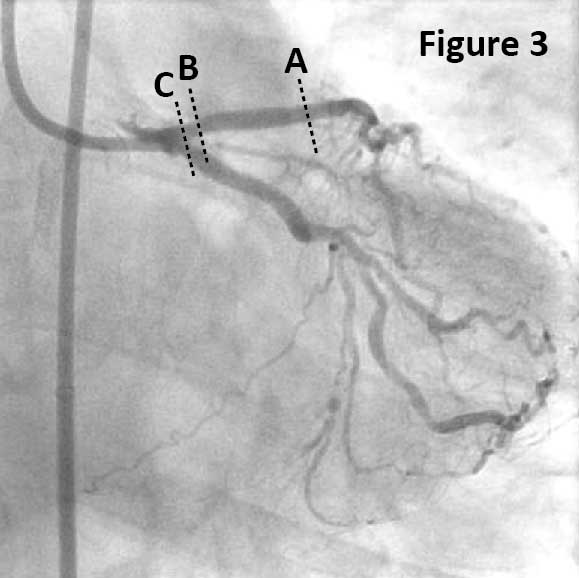
Rotational atherectomy with 1.75 mm burr was performed in the LCx lesion, while in-stent restenosis in the LAD was treated with cutting balloon. After lesion preparation, minicrush technique to LM bifurcation was performed with LM-LCX 3.0×24 mm and LM-LAD 3.5×20 mm DES followed by final kissing balloon inflation. Final angiography showed TIMI3 flow in both main vessel and side branches (Figure 3).
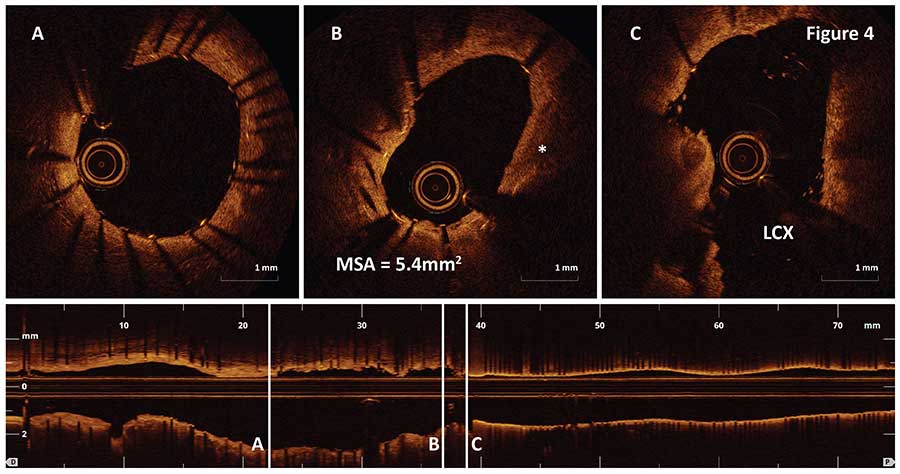
Post-PCI OCT imaging confirmed good stent apposition and expansion with MSA of 5.4mm2 even around calcifications (Figure 4B, asterisk) without dissection at the stent distal edge (Figure 4A) or around LCx ostium (Figure 4C).
Ask the Experts

Ask the Experts
We are ready to help you.
ask now
ask now
Take Quiz

Take Quiz
Know about OCT? Test your knowledge.
try it now
try it now
Meet the Team

Meet the Team
Read about the team behind the apps.
learn more
learn more
Contact Us

Contact Us
Reach out to us with general comments or questions.
connect now
connect now