










OCT Guided Calcified Bifurcation PCI
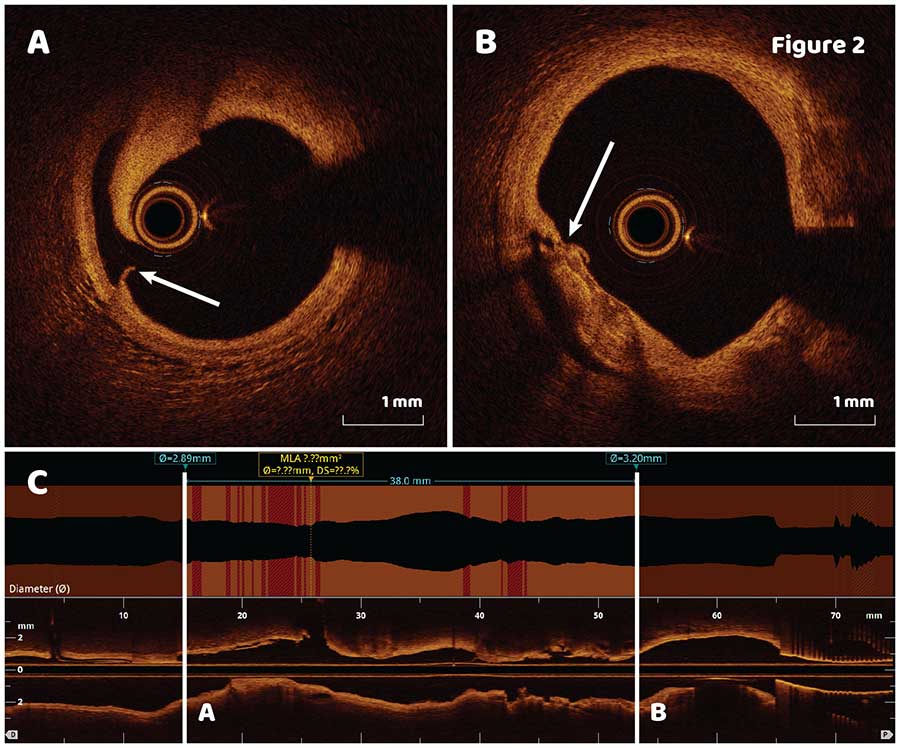
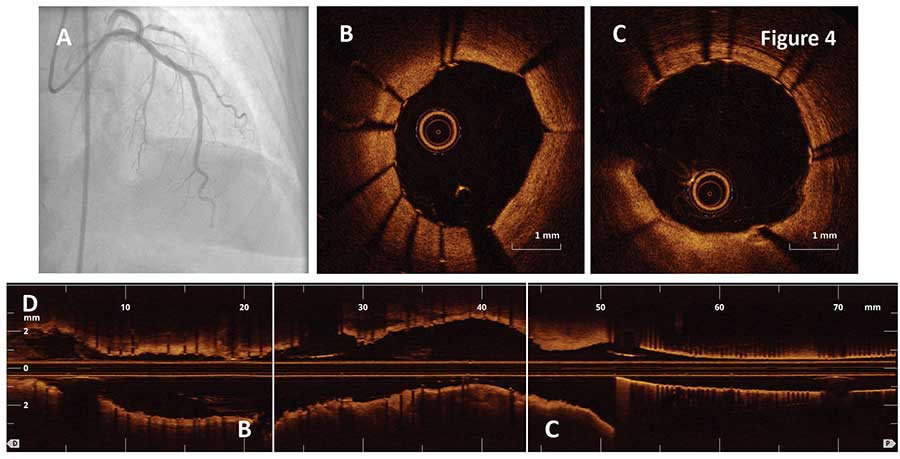
Quick longitudinal lesion assessment showed that the most distal and proximal cuts would not be covered by a 38 mm stent (Figure 2C), therefore a 2 stent approach was selected for the lesion. Second OCT pullback performed after the first 3.5 X 38 mm stent was implanted distally (Figure 3A) demonstrated no distal edge dissection (Figure 3B) and stent malapposition in the middle of the stent with stent area of 8.8 mm2 (Figure 3C). Minimal stent area and stent expansion was 5.6 mm2 and 74% respectively. Sizing of the second proximal stent using automatic lumen profile feature is shown in the longitudinal OCT view (Figure 3D, dotted line square). Based on the findings, a 3.5 X 16 mm stent was deployed to the proximal LAD followed by a postdilation of the distal stent with a 3.75 X 15 mm noncompliant balloon to resolve stent malapposition (Figure 4A).

Ask the Experts

Ask the Experts
ask now
Take Quiz

Take Quiz
try it now
Meet the Team

Meet the Team
learn more
Contact Us

Contact Us
connect now