










Plaque Rupture in NSTEMI
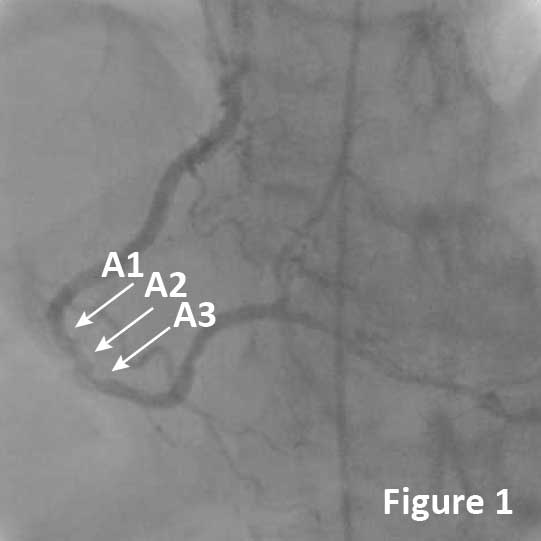
A 49-year-old male, ex-smoker with a history of prior myocardial infarction, hyperlipidemia, controlled hypertension, and controlled diabetes mellitus presented with a non-ST-elevation myocardial infarction (NSTEMI). Cardiac enzymes were elevated with cTnI 8.68 ng/mL and a small apical thrombus was identified by echocardiography. Coronary angiography showed a 90-95% stenosis with a filling defect in the distal RCA (Figure 1, arrows).
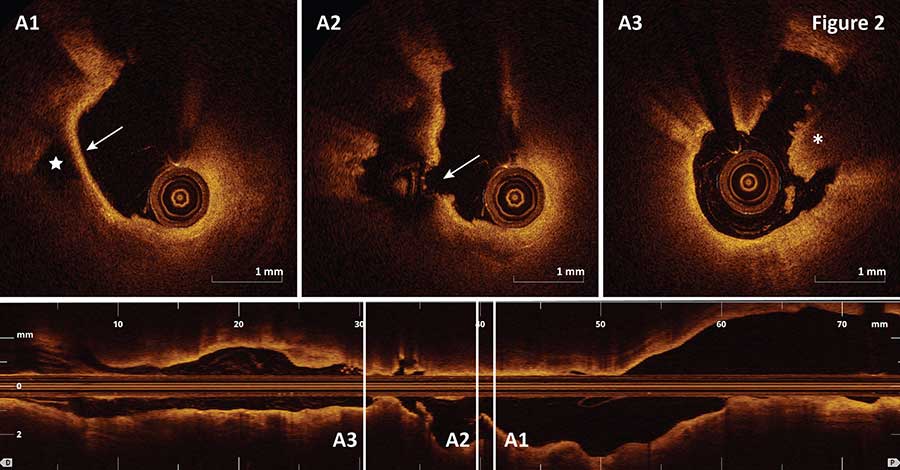
OCT imaging of the segment revealed the presence of plaque rupture (Figure 2A2, arrow), and an intact thin fibrous cap (Figure 2A1, arrow) overlying a ruptured plaque cavity (Figure 2A1, star) was visualized proximal to the site of rupture (Figure 2A2, arrow). In addition, large red thrombus was detected by OCT distal to the site of plaque rupture (Figure 2A3, asterisk).
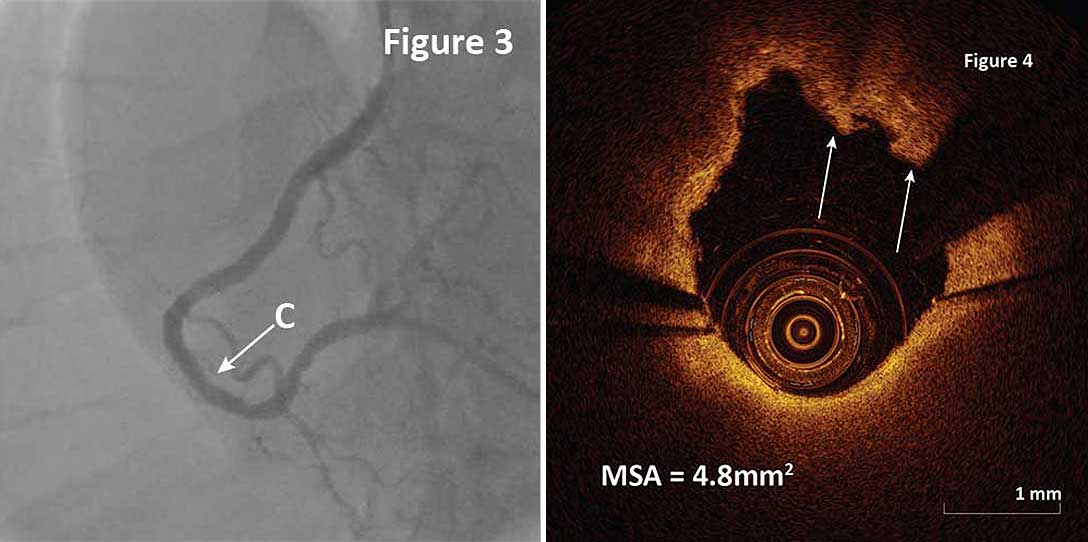
A 3.5x28mm DES was implanted in the culprit lesion with satisfactory angiographic result (Figure 3). Post-stent OCT pullback confirmed good stent apposition and expansion minimal stent area (MSA) of 4.8mm2. Small tissue protrusions were detected at the site of MSA (Figure 4, arrows). Acute plaque rupture was identified as an underlying mechanism for ACS in the case based on OCT before PCI and post-PCI OCT helped verify optimal stent expansion and apposition.
Ask the Experts

Ask the Experts
We are ready to help you.
ask now
ask now
Take Quiz

Take Quiz
Know about OCT? Test your knowledge.
try it now
try it now
Meet the Team

Meet the Team
Read about the team behind the apps.
learn more
learn more
Contact Us

Contact Us
Reach out to us with general comments or questions.
connect now
connect now