










Rotational Atherectomy of Calcified Left Main and LAD Lesions
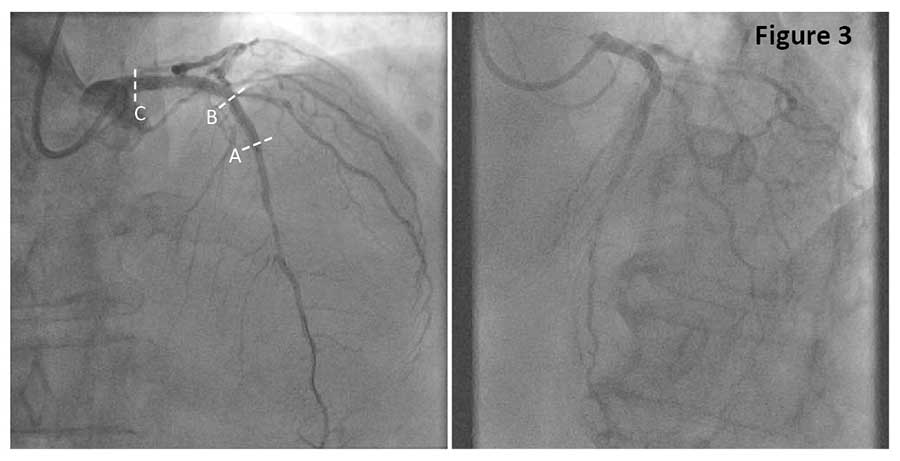
A 58-year-old male, who presented with unstable angina and underwent PCI of acutely occluded RCA three weeks earlier, now presents for a staged PCI of the LM and LAD. Coronary angiography before PCI showed a 50-60% stenosis of the distal LM and 80-90% bifurcation lesion in the LAD with 30-50% stenosis in the D2 branch (Figure 1). Moderate to severe calcification was detected by angiography in both, LM and LAD lesions.

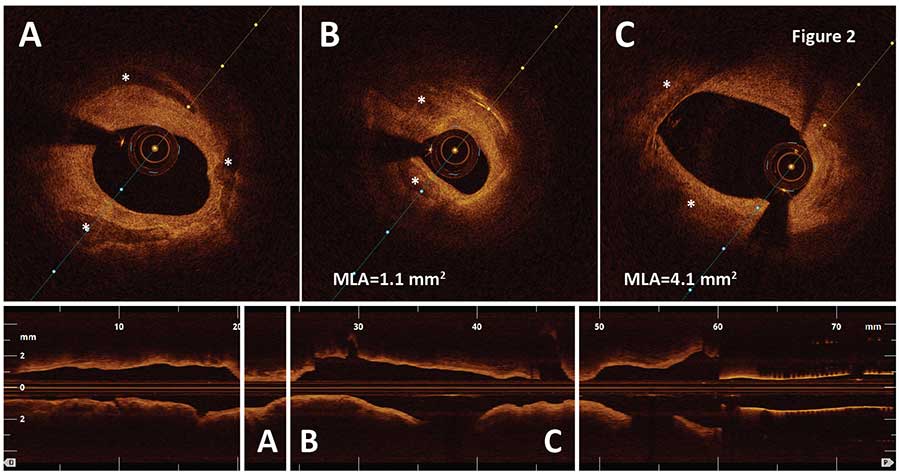
OCT pullback was performed in the LM and proximal LAD using a fast survey mode. The pullback detected circumferential calcification in the LAD lesion (Figure 2A, B, asterisks) with minimal lumen area (MLA) of 1.1 mm2 and a fibrocalcific plaque in the distal LM lesion, MLA = 4.1 mm2 (Figure 2C). Calcified plaques were ablated by rotational atherectomy (RA) using 1.75 mm burr in the LM and 1.5 mm burr in the LAD for 40 sec at 150,000 rpm.
Lesion modification with RA was followed by an implantation of two everolimus-eluting stents, 4/20 mm and 3.5/28 mm with a successful angiographic result (Figure 3).
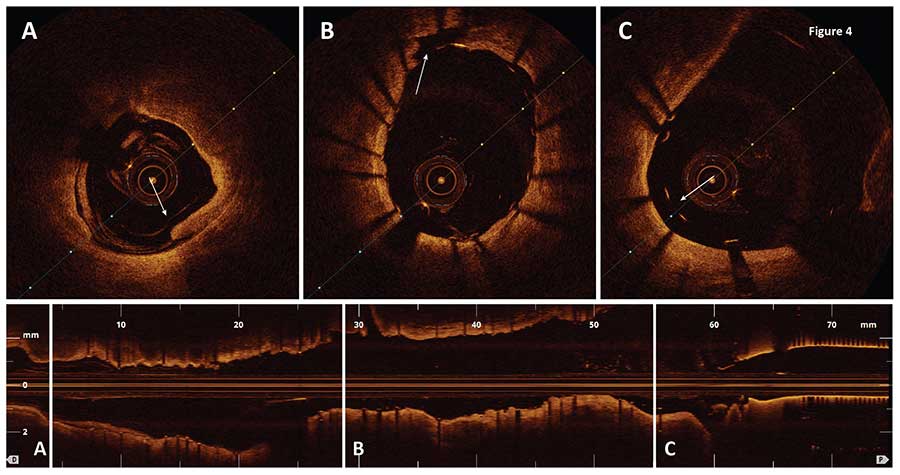
Postinterventional OCT imaging confirmed satisfactory expansion of both stents with minimal stent area (MSA) of 8.8 and 6.7 mm2 in the LM and LAD. A small dissection was detected at the distal edge of the LAD stent (Figure 4A, arrow). In addition, several malapposed struts were observed around a post RA tissue dissection in the LAD stent (Figure 4B) and at the proximal edge of the LM stent (Figure 4C). The OCT findings were considered minor and not waranting an additional stent optimization.
Ask the Experts

Ask the Experts
We are ready to help you.
ask now
ask now
Take Quiz

Take Quiz
Know about OCT? Test your knowledge.
try it now
try it now
Meet the Team

Meet the Team
Read about the team behind the apps.
learn more
learn more
Contact Us

Contact Us
Reach out to us with general comments or questions.
connect now
connect now