










Rotational Atherectomy of In-Stent Restenosis
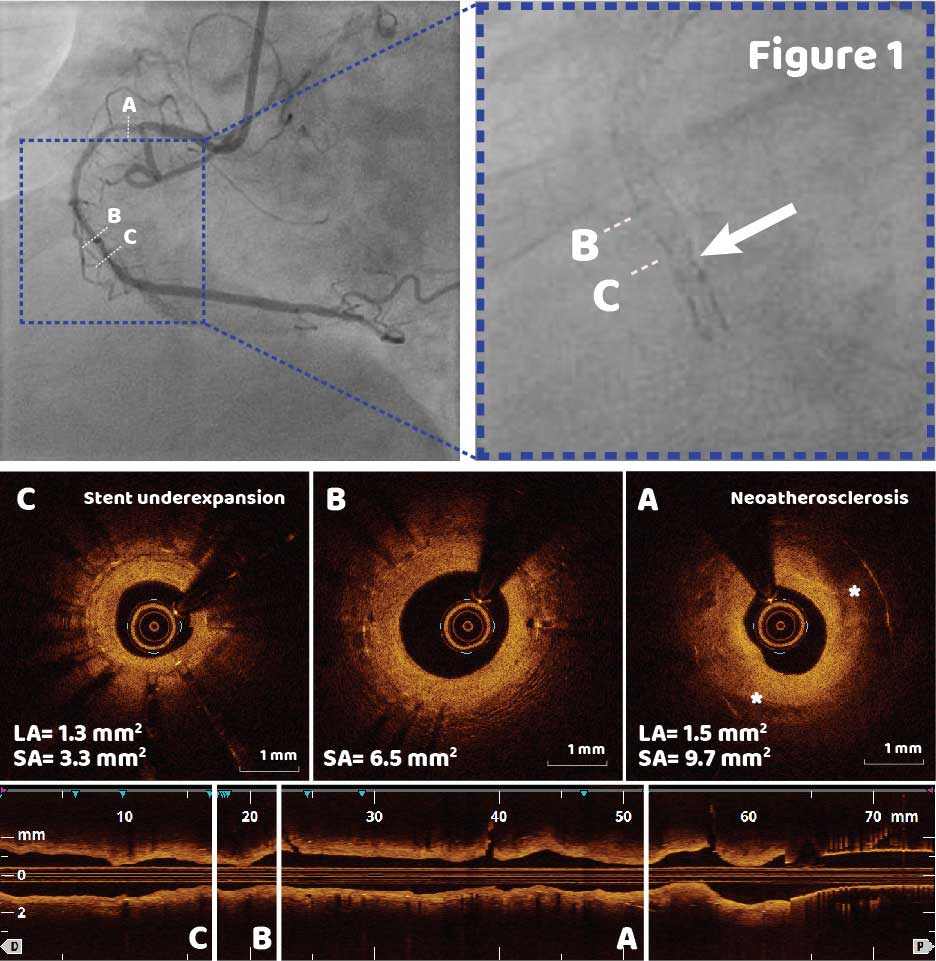
A 75-year-old patient with multiple previous PCIs including 2 second generation DES to the RCA, presented for elective PCI for the recurrent ISR. Coronary angiogram showed a 70-80% stenosis in both proximal and mid segment of the RCA (Figure 1); underexpansion of the stent implanted into the mid RCA was suspected based on angiography (Figure 1, arrow in the inset).
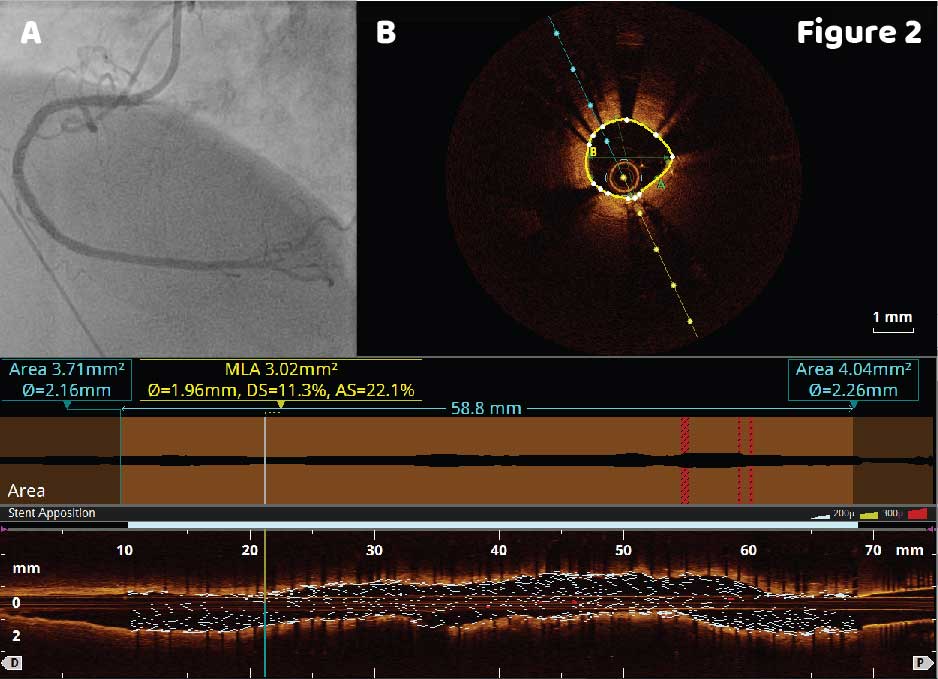
Based on OCT findings, the mid RCA lesion was treated using rotational atherectomy (RA) with a 1.5 mm burr; a combination of RA and atherotomy was used in the proximal RCA. A 3.5 X 33 mm DES was implanted in the proximal RCA, and a 3 X 38 mm was deployed to the mid RCA (Figure 2A). Post-PCI OCT showed well apposed stent struts and a satisfactory 78% relative stent expansion.
While rates of ISR defined as a luminal narrowing with >50% diameter stenosis of a stented coronary segment (or within 5mm of a stent edge) have declined with the use of DESs, ISR still accounts for 10% of PCI and the optimal treatment for DES-ISR remains unknown.1 Intracoronary imaging is critical to identify the mechanism of ISR and select an appropriate treatment modality by characterizing the presence of underexpansion or fracture, neointimal hyperplasia, neoatherosclerosis, and calcification. OCT’s diagnosis of stent underexpansion and neoatheroclerosis as the main mechanisms of ISR in this complex case helped select an appropriate lesion preparation strategy and achieve optimal post-PCI results.
References
1 Shlofmitz E, Iantorno M, Waksman R. Restenosis of Drug-Eluting Stents. Circ Cardiovasc Interv. 2019 Aug;12(8)
1 Shlofmitz E, Iantorno M, Waksman R. Restenosis of Drug-Eluting Stents. Circ Cardiovasc Interv. 2019 Aug;12(8)
Ask the Experts

Ask the Experts
We are ready to help you.
ask now
ask now
Take Quiz

Take Quiz
Know about OCT? Test your knowledge.
try it now
try it now
Meet the Team

Meet the Team
Read about the team behind the apps.
learn more
learn more
Contact Us

Contact Us
Reach out to us with general comments or questions.
connect now
connect now