










STEMI from Plaque Erosion
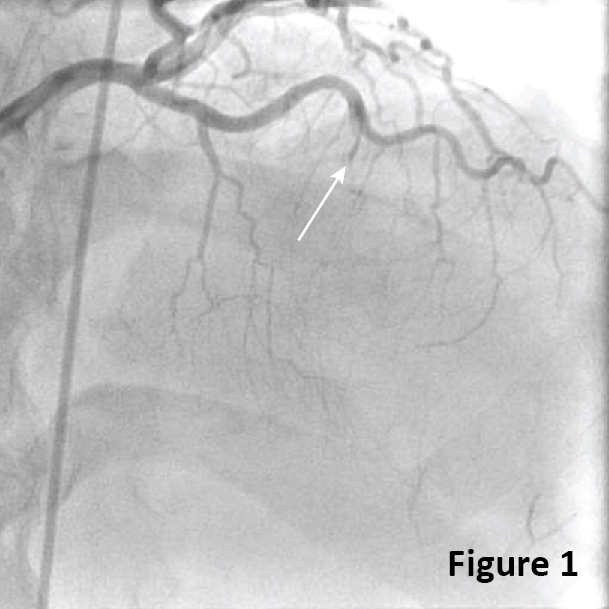
A 59-year-old male with no medical history arrived at emergency department due to sudden onset of chest pain radiating to back and shoulder. The ECG showed ST-elevation in leads V2-3 and an emergent coronary angiography revealed a total occlusion of the mid LAD (Fig. 1, arrow).
After wiring the LAD, an angiogram demonstrated a significant stenosis and filling defects (Fig. 2, arrow) suggesting thrombus with TIMI 3 flow.
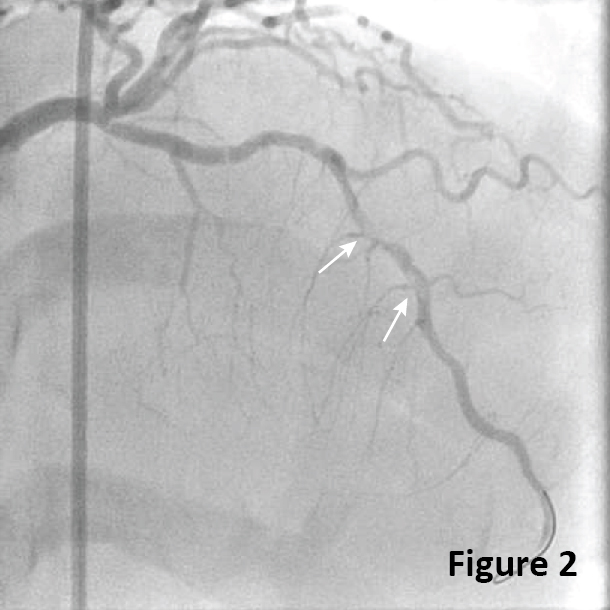
Figure 3 shows residual stenosis without obvious thrombus after thrombectomy and balloon angioplasty.
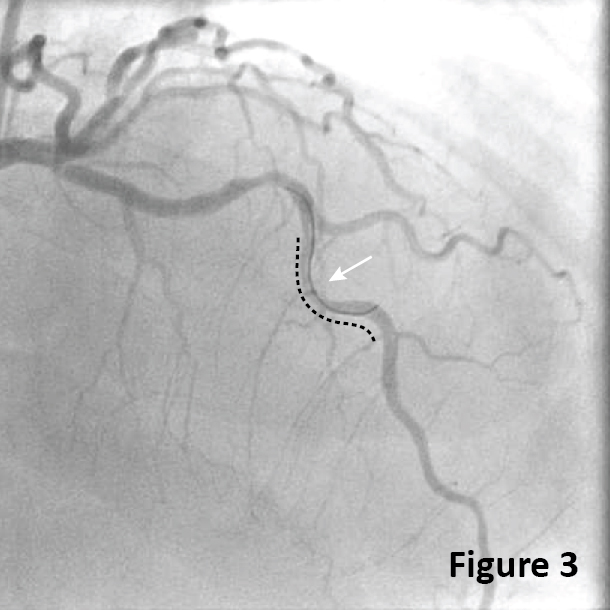
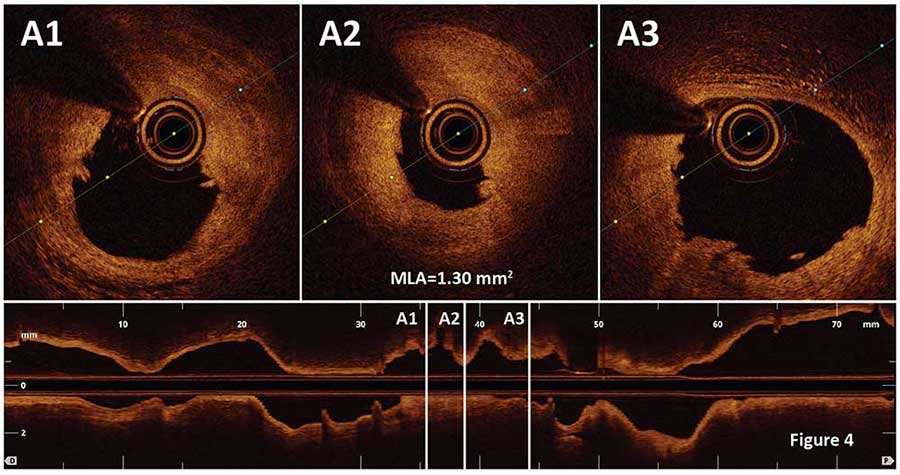
OCT was performed to uncover the underlying mechanism of STEMI (dotted line in Fig. 3). The OCT pullback demonstrated an irregular luminal surface with residual white thrombus overlaying fibrous plaque (Fig. 4A1, 4A3). Minimal lumen area (MLA) was 1.3 mm2 (Fig. 4A2). There was no plaque rupture or a lipid rich plaque detected in the lesion by OCT, suggesting plaque erosion as an underlying mechanism of STEMI (Video 1).
The obstructive lesion was treated by deploying a 3.0/28-mm drug eluting stent (Fig. 5)
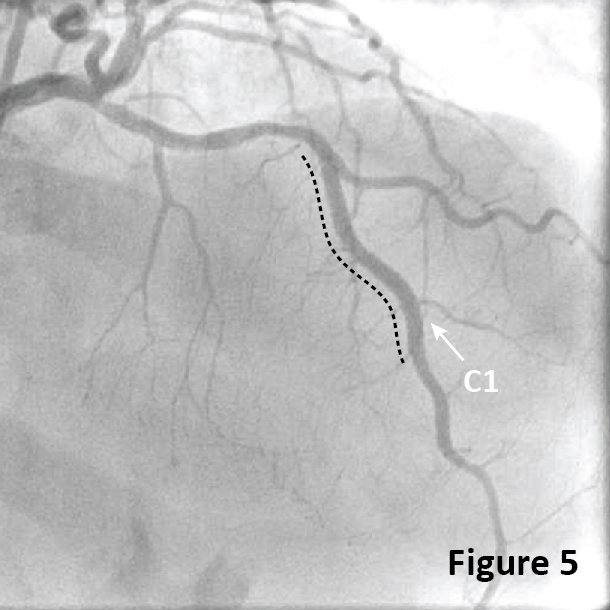
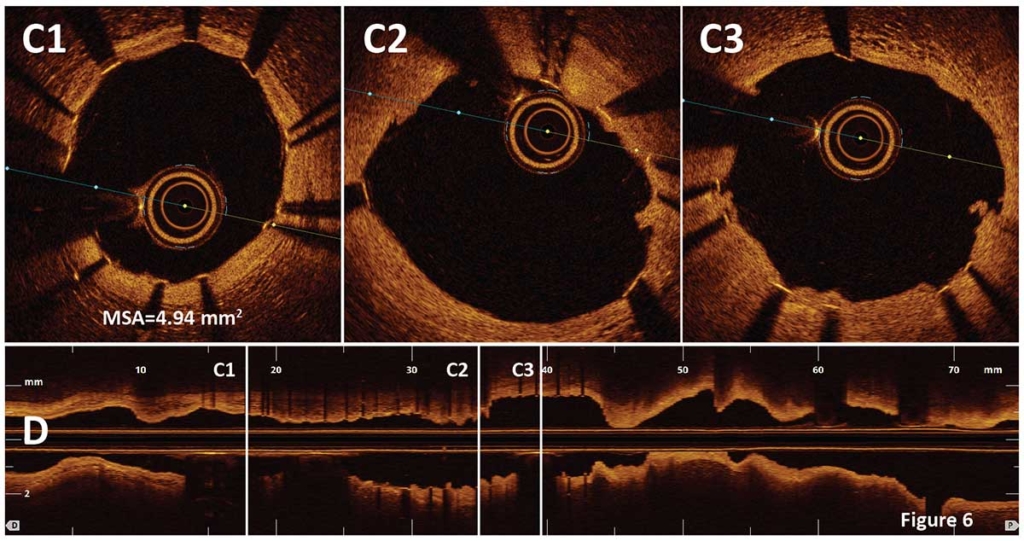
Post stent OCT (dotted line in Fig. 5) confirmed good stent expansion and apposition with a minimal stent area (MSA) of 4.94 mm2 (Fig. 6, Video 2). Small white thrombi and tissue protrusions were also demonstrated by OCT (Fig. 6C2, 6C3)
Ask the Experts

Ask the Experts
We are ready to help you.
ask now
ask now
Take Quiz

Take Quiz
Know about OCT? Test your knowledge.
try it now
try it now
Meet the Team

Meet the Team
Read about the team behind the apps.
learn more
learn more
Contact Us

Contact Us
Reach out to us with general comments or questions.
connect now
connect now