










Dissection Type C – Case 1
Clinical Presentation
- 76-year-old female who presented with dyspnea.
Past Medical History
- HTN, HLD, Asthma, COPD, GERD, OA, CKD
- LVEF 54%
Clinical Variables
- Stress MPI: Moderate apical and mild anteroseptal defect with reversibility.
Medications
- Home Medications: Aspirin, Rosuvastatin, Olmesartan
- Adjunct Pharmacotherapy: Clopidogrel, Bivalirudin
Pre-procedure EKG

Angiograms
1 of 11
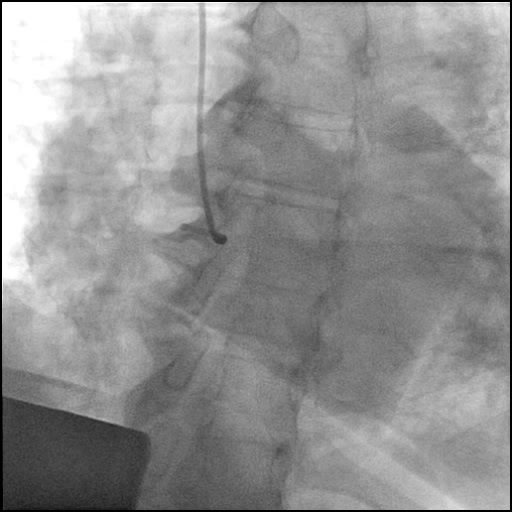
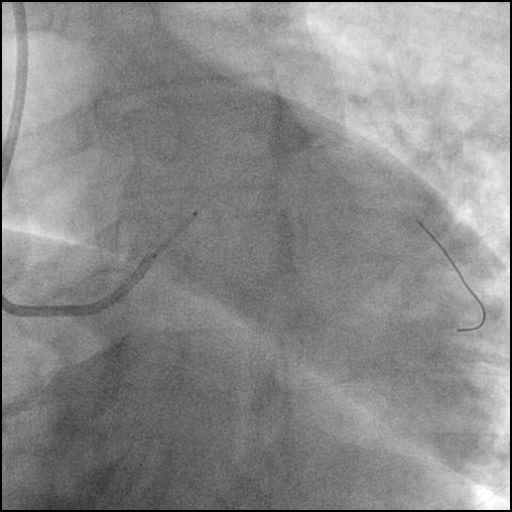
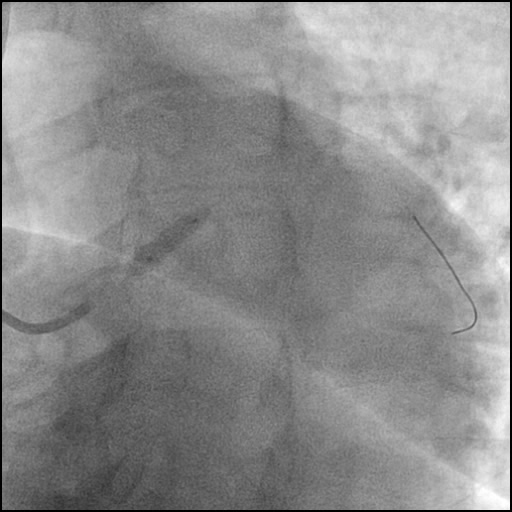
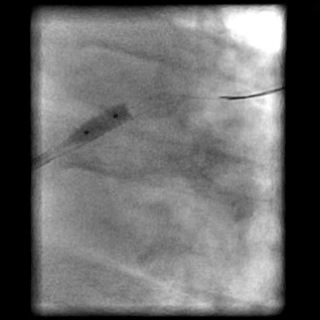
Right coronary artery (RCA) angiography 90% mid RCA lesion.
2 of 11
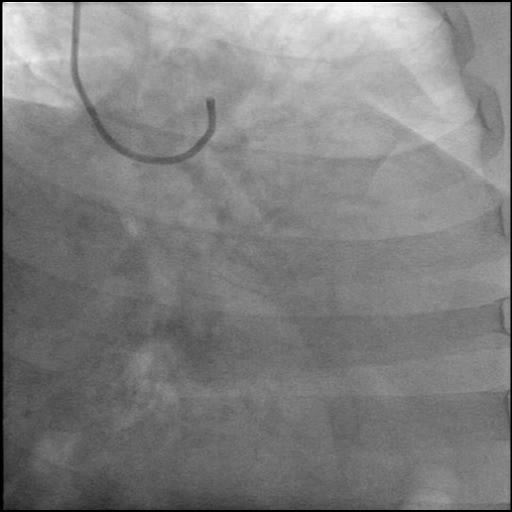
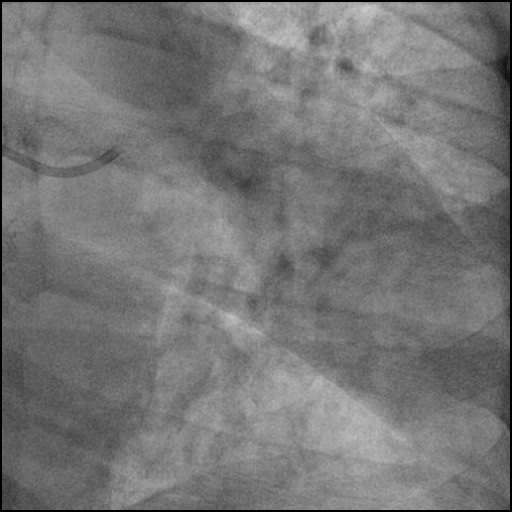
Left coronary artery angiography showing a guide catheter (VL…

3 of 11
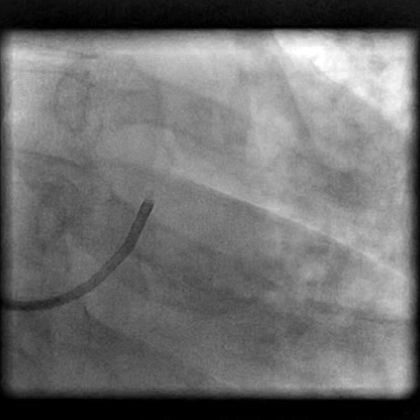
Guide catheter (VL 3.5/6 Fr) induced, non-flow limiting Type…
4 of 11
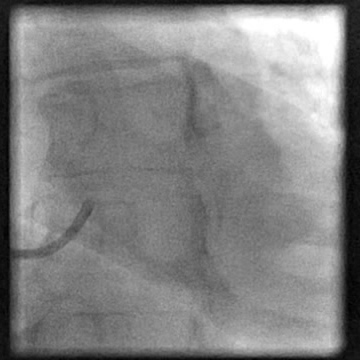
Guide catheter (VL 3.5/6 Fr), non-flow limiting induced Type…
5 of 11
LCA angiography performed after guide catheter exchanged to a…
6 of 11
LCA angiography performed after guide catheter exchanged to a…
7 of 11
Deployment of a Xience V 4.0/12 mm stent in…
8 of 11
Side branch (LCx) wired followed by post stent dilatation…
9 of 11
Angiography of the LM after stent post-dilatation showing presence…
10 of 11
Post dilatation of the stent placed in the LM…
11 of 11
Final angiography showing satisfactory treatment with a well contained…
Post-procedure EKG

Case Overview
- Underwent cardiac catheterization with difficulty engaging the LM osita with a diagnostic catheter (Tiger 5 Fr).
- Decision made to switch to a guide catheter (VL 3.5/6 Fr) to perform LCA diagnostic coronary angiography. However, this catheter caused traumatic injury, leading to a non-flow limiting Type C dissection of the LM.
- The patient remained hemodynamically stable throughout the procedure. For placement of an ostial LM stent, the VL guide was switched to a less aggressive guide catheter (FL 3.5/6 Fr) to avoid deep engagement, dissection propagation and further injury.
- Dissection was treated with direct stent placement followed by post-dilation of the stent.
- Residual contrast staining was seen underneath the stent. However, it appeared to be well contained with appropriate stent coverage; hence, further treatment was deferred.
- Troponin-I peaked at 0.1 ng/mL and CK-MB peaked at 0.7 ng/mL.
- Patient discharged home the following day without further sequelae.
Learning Objectives
- What is the likely explanation or reason why the complication occurred?
- Guide catheter induced injury of an angiographically normal LM.
- How could the complication have been prevented?
- Maintain guide catheter co-axiality, be cautious with manipulation of the guide catheter, and continuously monitor the position of the guide catheter throughout the procedure. This is extremely important when there is difficulty delivering equipment in tortuous, calcified, long type C lesions.
- Consider using a different guide catheter (smaller size, smaller curve, different curve).
- What are the important learning points?
- This is a type C dissection because of the persistence of extraluminal contrast seen well after contrast injection.
- It is reasonable to change the guide catheter which caused the dissection. However, this should only be done if there is difficulty keeping the guide catheter in a co-axial position, and if the clinical scenario allows.
- When a catheter is not in a co-axial position, be very cautious administering IC agents (medications, contrast, etc.) and avoid high pressure injections.
- Look at the pressure wave form prior to contrast injection; if the wave form is ventricularized or dampened, DO NOT INJECT. It is crucial to immediately disengage the guide catheter and take a non-selective injection of the vessel to rule out ostial disease.
- If a dissection is still present underneath the stent it means you can perform further post-dilation or even possibly increase balloon size to optimize post dilation.
- Remember to appropriately size the stent diameter and length to assure it adequately covers the entry and exit point of the dissection. We recommend routine LM intravascular imaging with IVUS to determine the optimal stent length, diameter, and landing zones. Intravascular imaging would have been particularly helpful in this case, in differentiating the etiology of a radiolucency seen during angiography.