










No Reflow – Case 1
Clinical Presentation
- 77-year-old male who presented with chest pain (CCS Class III) and was referred for IVBT.
Past Medical History
- HTN, HLD, CAD s/p 3-Vessel CABG followed by Multiple PCI’s, Atrial Fibrillation, Asthma, GERD, Esophagitis, Anemia
- LVEF 50%
Clinical Variables
- Prior Cardiac Catheterization: LIMA-LAD (occluded), SVG-D1 to D2 jump (patent), SVG-OM (occluded); mid LAD 70-80% stenosis, distal LCx CTO.
Medications
- Home Medications: Aspirin, Clopidogrel, Apixaban, Simvastatin, Ezetimibe, Carvedilol, Ranolazine, Aldactone, Furosemide, Tamsulosin, Gabapentin, Pantoprazole, Albuterol, Mometasone
- Adjunct Pharmacotherapy: Clopidogrel, Bivalirudin
Pre-procedure EKG

Angiograms
Previous
Next
1 of 15
Right coronary artery (RCA) angiography
- patent intervention site and no significant disease in the RCA.
1 of 15
Right coronary artery (RCA) angiography patent intervention site and…
2 of 15
Angiography of the SVG-D1 to D2 jump bypass graft…
3 of 15
Left coronary artery angiography 70-80% in-stent restenosis lesion in…
4 of 15
Wiring of the LAD with a Fielder wire and…
5 of 15
Rotational atherectomy of the LAD with a 1.75mm burr…
6 of 15
Angiography of the LAD after rotational atherectomy showing no-reflow.
7 of 15
IC vasodilators administered through the guide catheter without improvement…
8 of 15
Angiography of the LAD after PTCA showing minimal improvement…
9 of 15
PTCA of the LAD with a NC Emerge 3.0/8mm…
10 of 15
Angiography of the LAD after PTCA showing improved flow…
11 of 15
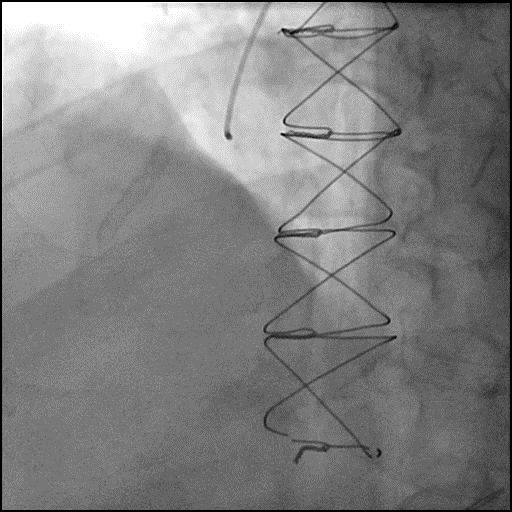
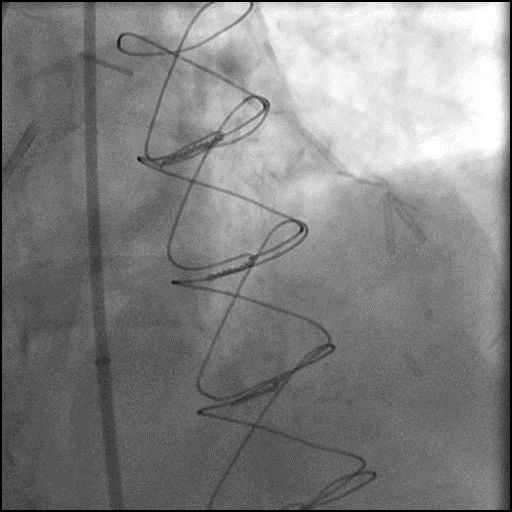
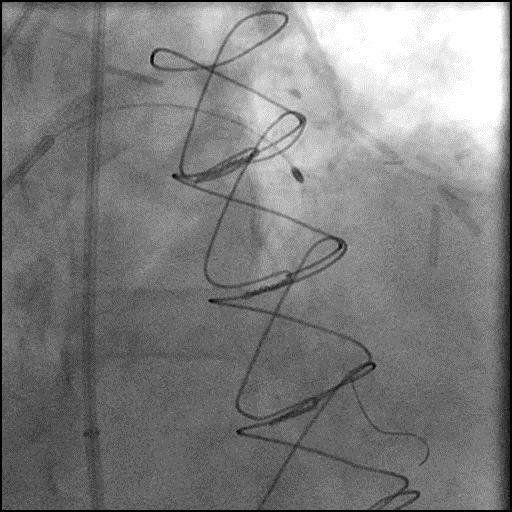
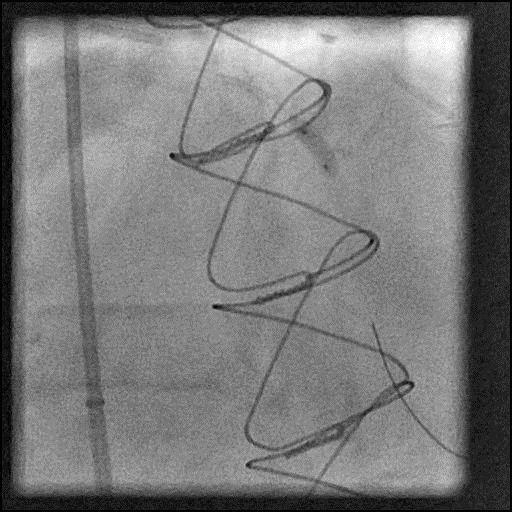
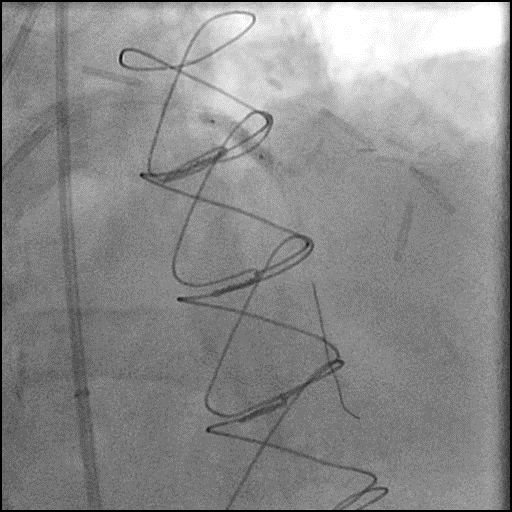
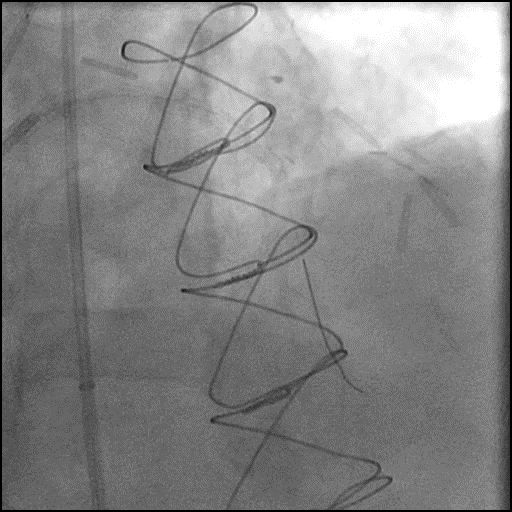
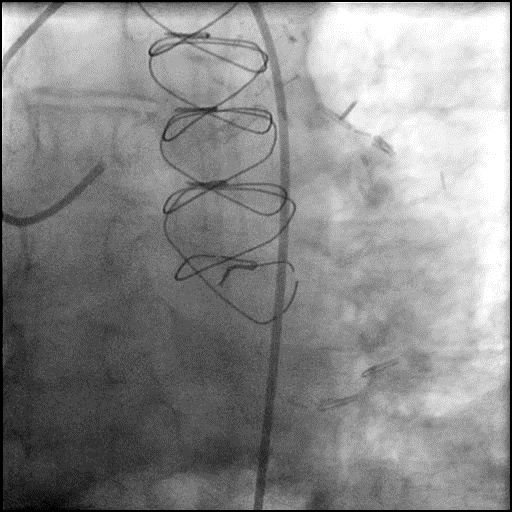
Delivery of IVBT source into the LAD.
12 of 15
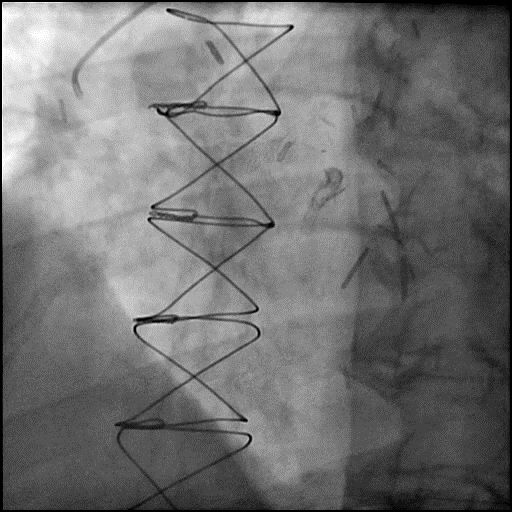
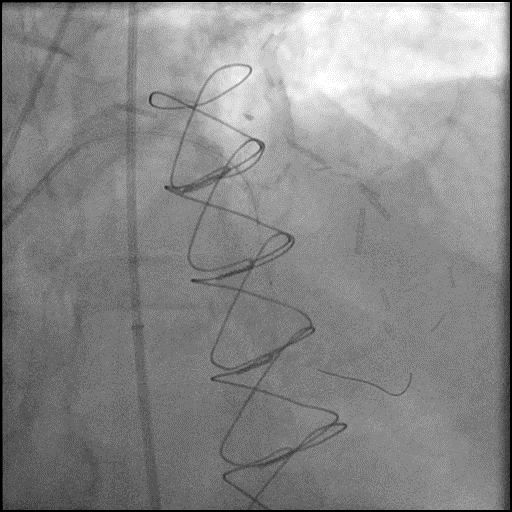
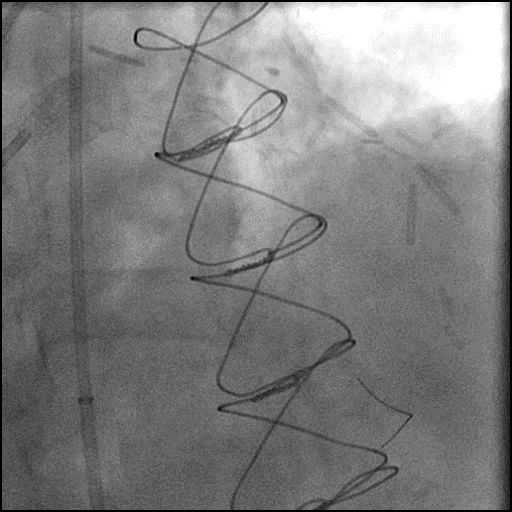
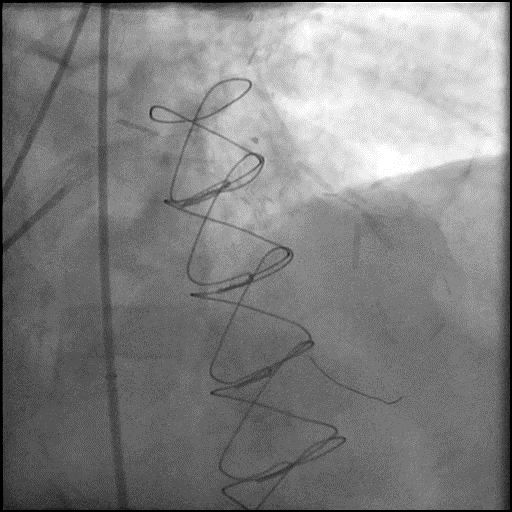
Post-IVBT angiography showing TIMI 2 flow.
13 of 15
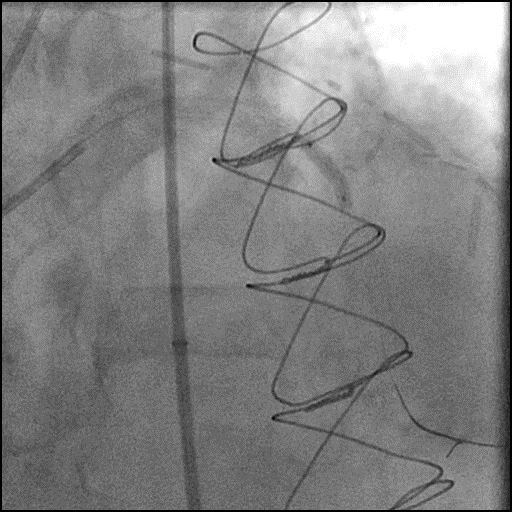
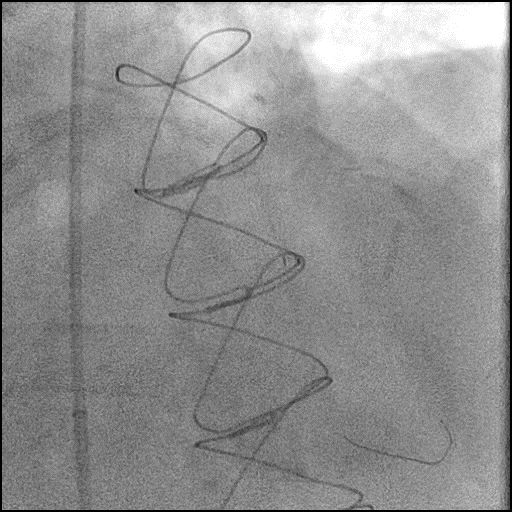
Repeat balloon dilatation of the LAD with a NC…
14 of 15
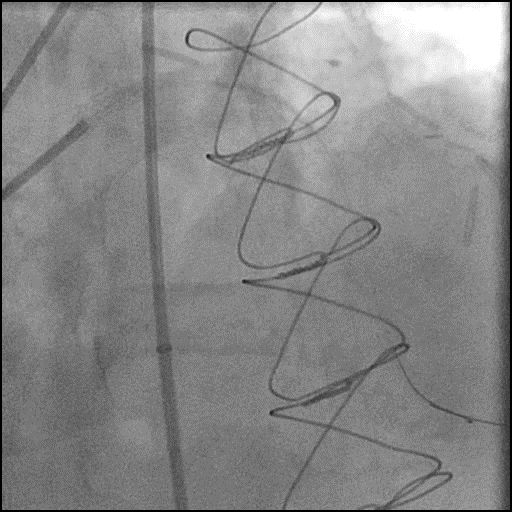
Angiography of the LAD after repeat balloon dilatation showing…
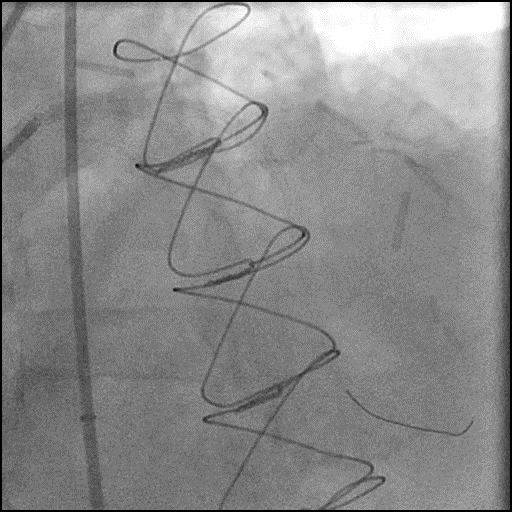
15 of 15
Final angiography of the LAD showing restoration of flow…
Post-procedure EKG

Case Overview
- Underwent intervention of the LAD.
- Procedure was complicated by no-reflow following rotational atherectomy.
- IC vasodilators administered without improvement in flow.
- PTCA was performed improving flow in the LAD.
- IVBT was performed followed by post-dilatation of the LAD.
- Troponin-I peaked at 15.99 ng/mL and CK-MB peaked at 94.4 ng/mL.
- Patient was discharged the next day without further sequelae.
Learning Objectives
- What is the likely explanation or reason why the complication occurred?
- No-reflow following rotational atherectomy – likely due to distal embolization of debris.
- How could the complication have been prevented?
- When performing rotational atherectomy consider the following to prevent complications:
- Keep systolic BP >100mmHg and avoid bradycardia
- Perform short runs <20 seconds with a gentle pecking motion to advance the rota burr, maintain rotational speed around 150-160k RPM
- Use Rota-flush and consider use of glycoprotein IIB/IIIA inhibitors
- Vasodilators should be given prophylactically and for treatment of slow flow/no-reflow.
- Assure patient is given adequate periprocedure antithrombotic therapy (antiplatelets and anticoagulants).
- Pay close attention to the ACT during the procedure and dose anticoagulation accordingly to maintain ACT >300 prior to performing an intervention (Hemochron machine).
- Use a rota-burr which is appropriately sized for the vessel. Ideally the burr should be 0.5-0.6x the distal vessel size when performing a plaque modification strategy, and 0.8-0.85x the distal vessel size when performing a debulking strategy (STRATA trial). With plaque modification strategy the purpose is to disrupt the calcium so it allows for safe passage of devices and easier expansion of device, balloons, and stents. With debulking, the aim is to break the calcium into particles so it can move through the coronary artery and eventually washout of the coronary microcirculation.
- When performing IVBT, additional anticoagulation is recommended prior to placing the IVBT catheter and delivery of source to the coronary vessel to help prevent thrombosis from prolong source dwelling time.
- Is there an alternate strategy that could have been used to manage the complication?
- The initial step in management of slow flow/no-reflow involves administration of intra-coronary vasodilators through the guide catheter. If this fails, recommended using a dual-lumen microcatheter (Twinpass is the only dual lumen microcatheter available in the USA) to deliver intra-coronary medications to the distal vessel and microvasculature. Next, perform angiography with delivery of contrast through the microcatheter to determine if there is distal coronary flow. If distal vessel flow is not preserved the likely etiology of abrupt vessel closure (AVC) is no-reflow due to distal embolization of debris or thrombus, and IC vasodilators should be administered through the microcatheter targeted to the distal vessel and microvasculature. If flow is preserved, then the likely etiology of AVC is dissection (proximal to the point of microcatheter injection), and treatment involves placement of a stent. It is reasonable to perform aspiration thrombectomy prior to microcatheter based angiography injection (depending on the clinical context/presence of thrombus).
- Consider using laser atherectomy but unlikely to be successful because of the severity of under-expanded stent which caused ISR.
- Use an CE-mark OPN balloon (not available in USA) can be useful in treatment of an under-expanded stent.
- What are the important learning points?
- The best treatment for slow flow/no-reflow is to prevent it from happening.
- The exact mechanism of the no-reflow phenomenon is unclear, but it is thought to be associated with endothelial swelling, neutrophil infiltration, and platelet aggregation causing obstruction and spasm in the microvasculature.
- One of the possible complications of PCI especially during rotational or orbital atherectomy is slow flow/no-reflow. The common settings where this complication arises are when performing interventions of long calcified lesions, CTO’s (particularly RCA CTO), thrombotic lesions, and vein grafts. Also, incidence is higher when a patient has poor LV function and hemodynamic instability.
- Important to have multiple vasodilators readily available during a procedure. We use the following agents and administer them intra-coronary:
- Nitroprusside 50-200 mcg, Adenosine 30-40 mcg, Verapamil 100-200 mcg, Nicardipine 100-200 mcg
- Nitroglycerin 100-200 mcg (we use NTG for slow flow/no-reflow when it involved the epicardial vessels and not the coronary microvasculature)
- If the patient is hypotensive and this impedes the administration of intra-coronary vasodilators to treat slow flow/no-reflow, we recommend administration of IV phenylephrine 100-200 mcg as needed (may result in reflex bradycardia) to increase blood pressure, and then administer intra-coronary vasodilators.
- If there is refractory slow flow/no reflow then consider placement of an IABP. This helps with reduction in afterload, and improves coronary perfusion pressure by increasing coronary blood flow during diastole, and reduction in LVEDP.
- Depending on the size and function of the LV (LVEF <30%), consider using upfront LV support as it can help improve coronary perfusion pressure.
- Use intracoronary imaging (IVUS/OCT) to identify the etiology of in-stent restenosis and plaque composition. In-stent restenosis lesions of DES are prone for slow flow following rotational atherectomy, particularly if in-stent restenosis is due to lipid rich neo-atherosclerosis.