










Dissection Type D – Case 1
Clinical Presentation
- 50-year-old male who presented with chest pain (CCS Class III).
Past Medical History
- HTN, HLD, DM, CAD s/p PCI, CVA, Active Tobacco Use, GERD
- LVEF 64%
Clinical Variables
- Stress MPI: Moderate-size reversible size perfusion defect involving the inferior and lateral segments.
Medications
- Home Medications: Aspirin, Simvastatin, Isosorbide Dinitrate, Enalapril, Omeprazole, Metformin
- Adjunct Pharmacotherapy: Clopidogrel, Bivalirudin
Angiograms
Previous
Next
1 of 8
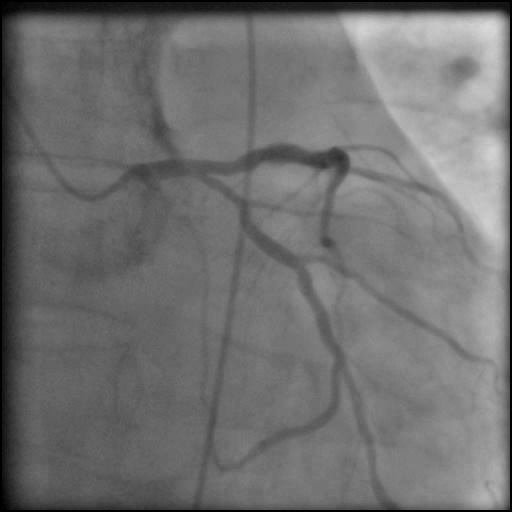
Left coronary artery angiography
- no significant lesions in the left anterior descending (LAD) and left circumflex (LCx) coronary arteries.
1 of 8
Left coronary artery angiography no significant lesions in the…
2 of 8
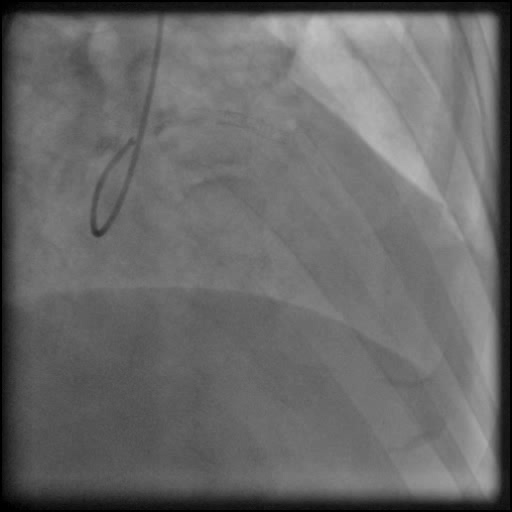
Right coronary artery (RCA) angiography chronically occluded proximal right…
3 of 8
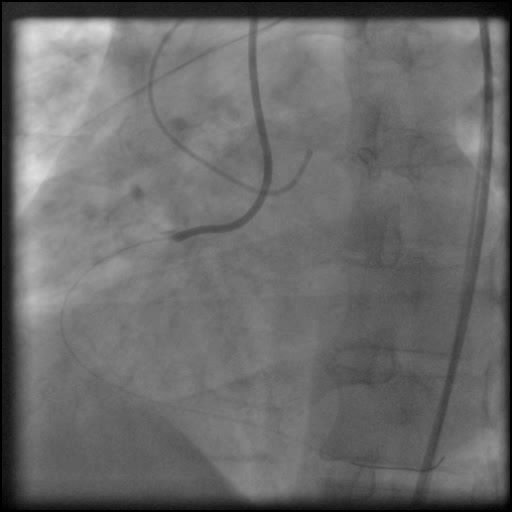
Dual injection of RCA and LCA showing collaterals from…
4 of 8
Successful wiring across RCA CTO.
5 of 8
Angiography of the RCA after traversing the CTO showing…

6 of 8
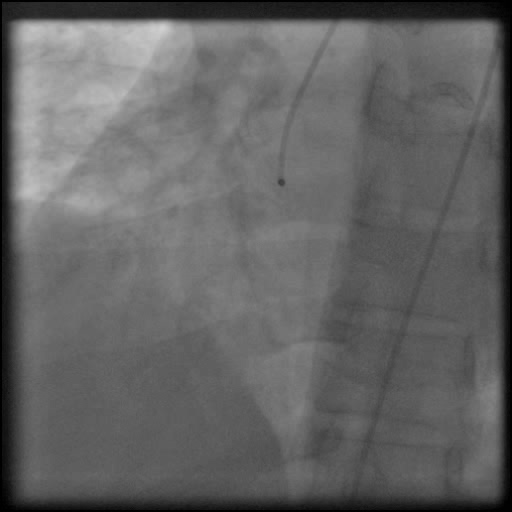
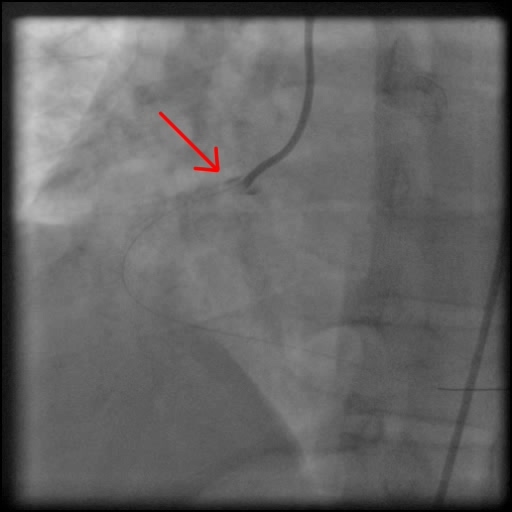
Angiography of the RCA showing contrast staining extending from…
7 of 8
LCA angiography showing contrast staining of the wall of…
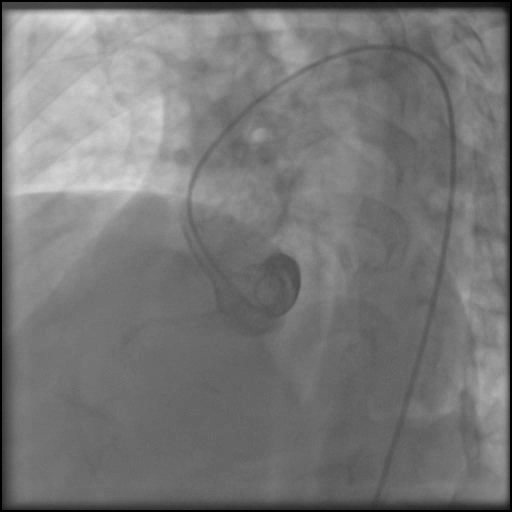
8 of 8
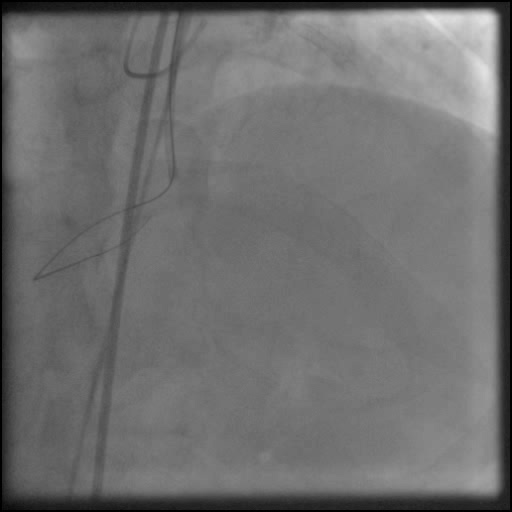
Aortogram performed with a pigtail catheter showing contrast staining…
Post-procedure EKG

Post-procedure Echocardiography
Case Overview
- Underwent unsuccessful intervention of the RCA CTO complicated by a guide catheter-induced, non-flow-limiting, Type C dissection of the ostial RCA with retrograde extension into coronary sinus and aorta, leading to a Type A aortic dissection.
- Patient remained hemodynamically stable; however, with severe chest pain.
- Procedure was aborted, and a Chest CT angiography was obtained emergently.
- Chest CT angiography showed a focal dissection at the origin of the RCA and coronary cusp. In addition, contrast material was seen extending superiorly/distally within the wall of the ascending aorta and aortic arch, concerning for dissection or hematoma.
- Transesophageal Echocardiography was performed, and no intimal flap was seen in the aorta. The findings were more consistent with an isolated RCA dissection.
- CT Surgery was consulted, and they recommend to continue with conservative therapy.
- Follow up CTA 3 days later showed small focus of intravenous contrast external to the aorta with significant improvement compared to the prior examination.
- Troponin-I peaked at 0.1 ng/mL and CK-MB peaked at 1.8 ng/mL.
- He was discharged home four days later without any sequelae.
Learning Objectives
- What is the likely explanation or reason why the complication occurred?
- Guide catheter induced injury of the RCA.
- How could the complication have been prevented?
- Maintain guide catheter coaxiality, be cautious with manipulation of the guide catheter, and continuously monitor the position of the guide catheter throughout the procedure. This is extremely important when there is difficulty delivering equipment in tortuous, calcified, long type C lesions.
- Consider using a different guide catheter (smaller size, smaller curve, different curve)
- What are the important learning points?
- This is a Type C dissection because of the persistence of extraluminal contrast seen well after contrast injection.
- Dissection of the ostial RCA and LM can propagate both antegrade and/or retrograde.
- When the dissection propagates retrograde it can extend into the coronary sinus and aorta behaving as an aortic dissection.
- If there is concern for retrograde extension of a dissection into the coronary sinus or aorta; perform an aortagram using a pigtail catheter.
- If the dissection flap extending into the aorta is less than 4 cm, conservative management is preferred.
- If larger than 4 cm post procedure cardiac CTA should be obtained to help guide further management.
- OCT imaging is useful to help guide further therapy.
- Echocardiography is also important to obtain in follow up to assess if a pericardial effusion has developed and assess the aorta for possible dissection.
- Usually stenting of the ostium of the vessel involved typically treats the dissection flap preventing further progression but this is not always the case.
- If there is a significant aortic dissection > 4 cm, AI, pericardial effusion an urgent/emergent CTS consult should be placed.