










Case 1: Distal LM calcified bifurcation treated with two-stent approach
Case Presentation
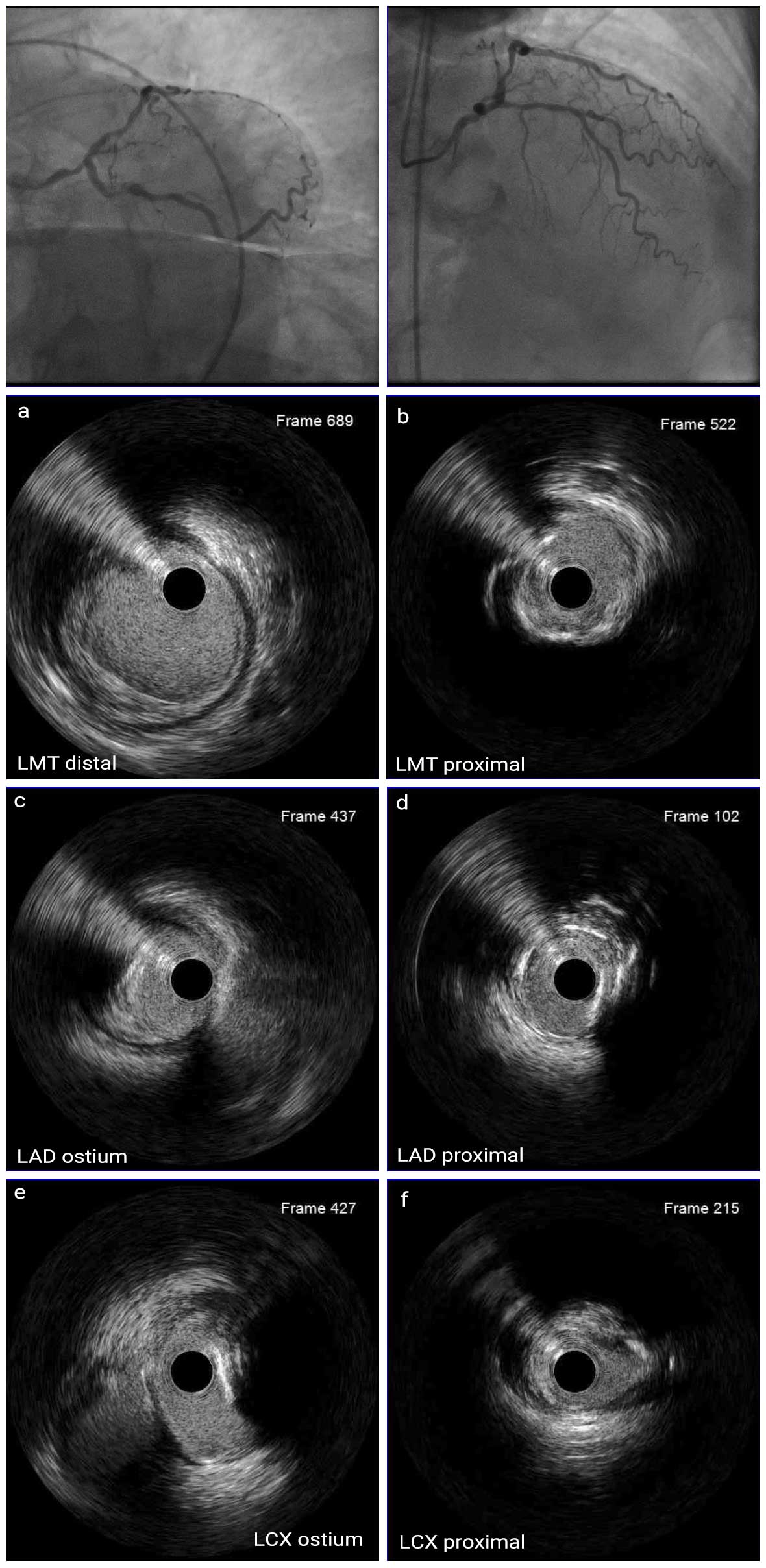
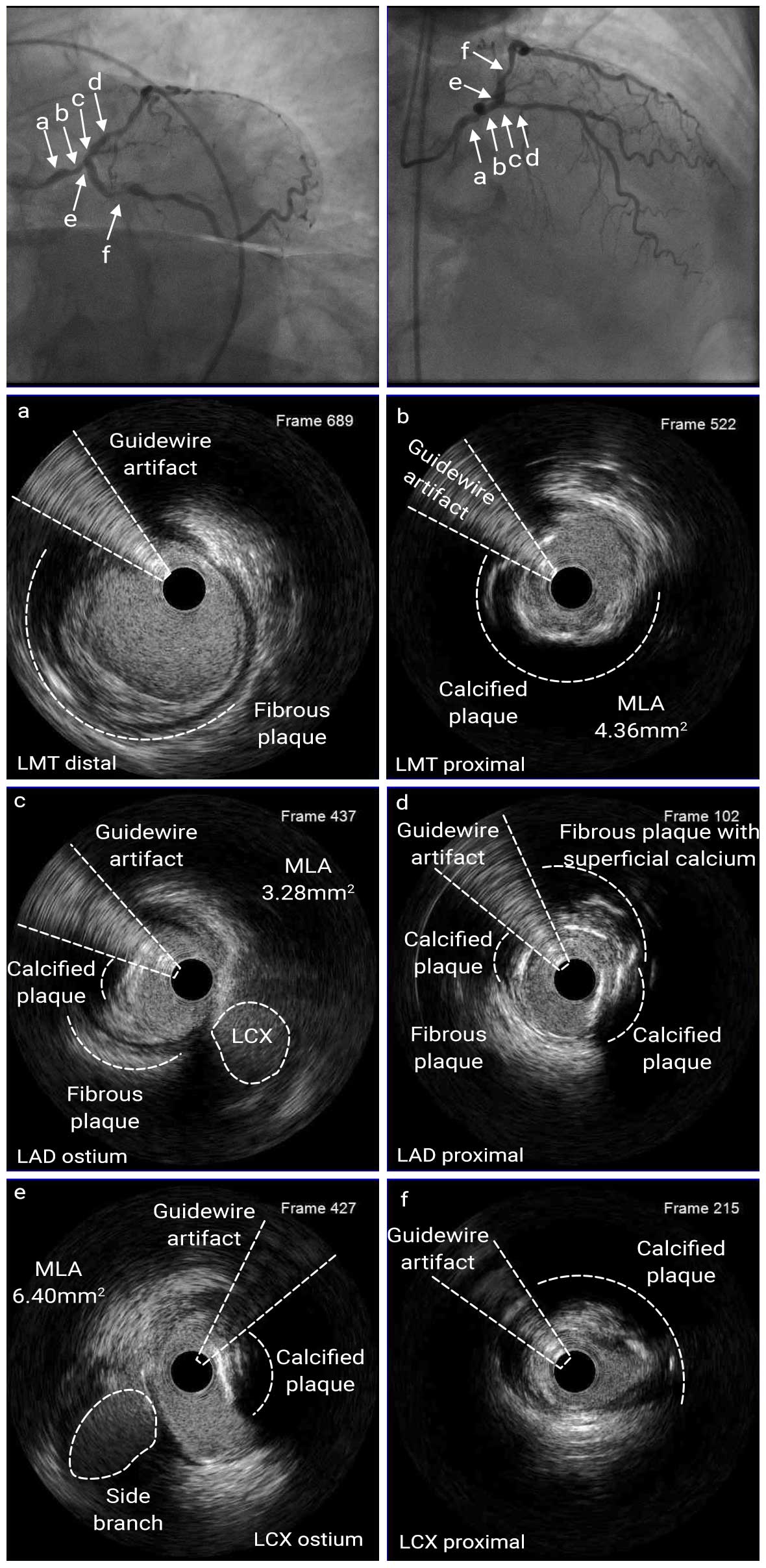
A 68-year-old female presented with new onset CCS Class III angina and positive SPECT MPI for multi-vessel ischemia. A coronary angiography revealed multi-vessel CAD with 80% stenosis at the distal LM, 70% stenosis at the proximal LAD (d), 90% stenosis at the proximal LCX (f), and 95% stenosis at the proximal RCA, and 90% stenosis at the RPDA with SYNTAX Score of 32. Prior to this PCI, RCA PCI had already been done. She had a history of hypertension, diabetes mellitus, and hyperlipidemia. Echocardiography showed normal left ventricular wall motion with ejection fraction of 64%.
Angio Pre
IVUS Pre LAD run
IVUS Pre LCX run
IVUS images showed that the LM lesion had a 180° arc superficial calcified lesion, and the proximal LM had a lumen diameter of 3.8mm. The MLA were 4.36mm2, 3.28mm2, and 6.40mm2 for distal LM, ostial LAD and ostial LCX, respectively. The stenosis of ostial LCX was not significant by angiography or IVUS, but IVUS showed calcified plaque. In addition, IVUS image revealed the stenosis at the ostial LAD. Therefore, we pre-dilated the lesion in LM and LAD with 3.0mm cutting balloon, and then 3.5mm non-compliant balloon was used for the lesion in LM, LAD, and LCX. A Mini-crush stenting was performed with 3.5mm x 38mm DES at the LAD-LM and 3.0mm x 32mm DES at the LCX-LM. The stents were post-dilated with 4.0mm NC balloon in the LAD-LM and 3.0mm NC balloon in the LCX. Finally, KBI was performed by using 3.5mm NC balloon in LAD and 3.0mm NC balloon in LCX. The MSA of LM, LAD, and LCX was 11.1mm2, 8.5mm2, 7.6mm2, respectively.


IVUS Post LAD run
IVUS Post LCX run
Angio Post
In this case, the lesion appeared to be a bifurcation lesion with a Medina classification of (1,0,0) on angiography, but IVUS revealed stenosis of the ostial LAD and patient was treated with a 2-stent technique. Post-stent IVUS confirmed optimal stent expansion and apposition.
IVUS-guided stent optimization has been shown to improve long-term outcomes in patients with LM bifurcated lesions with the following cut-offs for the MSA: LCX ≥ 5mm2, LAD≥6mm2, LM ≥ 8mm2.1

- Kang SJ, Ahn JM, Song H, et al. Comprehensive intravascular ultrasound assessment of stent area and its impact on restenosis and adverse cardiac events in 403 patients with unprotected left main disease. Circ Cardiovasc Interv. 2011;4:-562-569.