

































Case 13: Ostial LCx stenting and stent sizing
Case Presentation
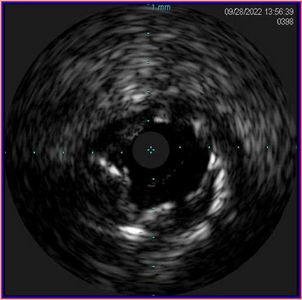
A 75-year-old male presented with new onset CCS class III angina. The patient had a history of PCI with two stents implanted in the proximal and mid LAD. Coronary angiography revealed a 90% lesion in the ostial LCx. IVUS images showed fibrofatty and calcified plaque with MLA of 2.3mm² in the ostial LCx. There was no healthy segment distal to the lesion, and we selected a segment with minimal plaque burden as a distal landing zone. The average vessel diameter was 4.9mm (EEL-EEL) and the average lumen diameter was 3.5mm. Proximal reference was not obtained due to ostial nature of the lesion. The catheter’s (Eagle Eye Platinum) markers with 10mm spacing were used to estimate the length of the stent. Based on IVUS quantitative measurements and qualitative plaque assessment at the site of stenosis and landing zone, we decided to perform pre-dilation with 3.5mm non-compliant (NC) balloon and use a 3.5 x 18mm DES for stenting.


Pullback Pre-Stent
Repeat IVUS after stenting revealed jailed struts of the previously implanted stent in the ostial LAD, therefore, we performed post-dilatation using 3.5mm NC balloon followed by a KBI with 3.5mm NC balloon in the LAD and 3.5mm NC balloon in the LCx.


Final IVUS pullback performed from the LAD to LM showed no residual side branch jailing at the polygon of confluence (POC); LAD ostium after KBI was MSA was 8.0mm².


Pullback Post Stent LAD-LM
Pullback Post Stent LCx-LM
In this case, IVUS was used to select treatment strategy and stent size in ostial LCx PCI. Post-stent IVUS detection of jailed struts in the LAD led to the use of KBI for post-stent optimization.